


Atrioventricular (AV) block is partial or complete interruption of impulse transmission from the atria to the ventricles. The most common cause is idiopathic fibrosis and sclerosis of the conduction system. Diagnosis is by electrocardiography; symptoms and treatment depend on degree of block, but treatment, when necessary, usually involves pacing.
(See also Overview of Arrhythmias.)
The most common causes of AV block are (1)
Idiopathic fibrosis and sclerosis of the conduction system (about 40% of patients)
Ischemic heart disease (20%)
The remaining cases of AV block are caused by
Medications (eg, beta-blockers, calcium channel blockers, digoxin, amiodarone)Medications (eg, beta-blockers, calcium channel blockers, digoxin, amiodarone)
Increased vagal tone
Valvulopathy
Congenital heart, genetic, or other disorders
Up to one-third of patients age 18 years to 60 years with new-onset Mobitz II second-degree or third-degree AV block without evident structural heart disease are diagnosed with cardiac sarcoidosis after targeted investigations (2).
Transient or reversible causes of AV block can include Lyme carditis and neurologically mediated (vagal) heart blocks.
Atrioventricular block may be partial or complete. First-degree and second-degree blocks are partial. Third-degree blocks are complete.
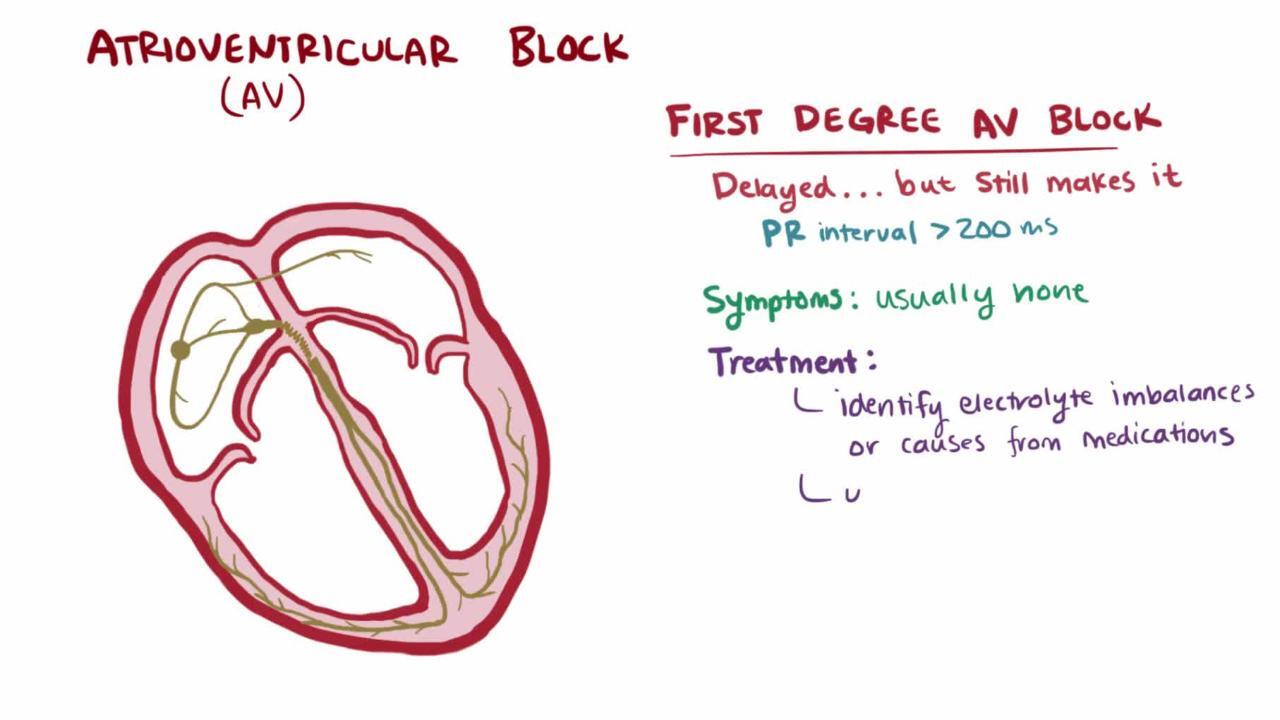
First-degree AV block
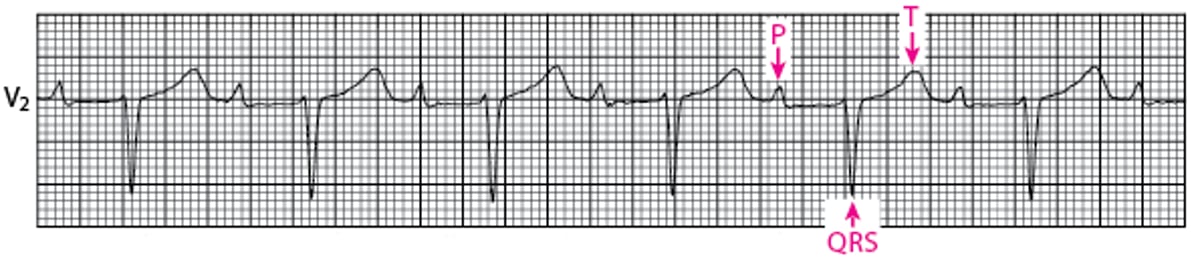
All normal P waves are followed by QRS complexes, but the PR interval is longer than normal (> 0.20 second—see figure First-Degree Atrioventricular Block).
First-Degree Atrioventricular Block
For first-degree block, conduction is slowed without skipped beats. All normal P waves are followed by QRS complexes, but the PR interval is longer than normal (> 0.2 second). |

First-degree AV block may be physiologic in younger patients with high vagal tone and in well-trained athletes. First-degree AV block is rarely symptomatic, and usually no treatment is required. When the PR interval is very long (> 0.3 second), exercise intolerance due to dyspnea or fatigue may occur due to loss of AV synchrony.
Further investigation may be indicated when first-degree AV block accompanies another heart disorder or appears to be caused by medication.
Second-degree AV block
Some normal P waves are followed by QRS complexes, but some are not. Two types exist:
Mobitz type I
Mobitz type II
In classic Mobitz type I second-degree AV block, the PR interval progressively lengthens with each beat until the atrial impulse is not conducted and the QRS complex is dropped (Wenckebach phenomenon); AV nodal conduction resumes with the next beat, and that beat has the shortest PR interval; the sequence is repeated (see figure Classic Mobitz Type I Second-Degree AV block). Commonly, the PR interval prolongation during the sequence is more variable but then always shortens with the first conducted beat after the pause (3).
Classic Mobitz Type I Second-Degree Atrioventricular Block
The PR interval progressively lengthens with each beat until the atrial impulse is not conducted and the QRS complex is dropped (Wenckebach phenomenon); atrioventricular nodal conduction resumes with the next beat, which has the shortest PR interval, and the sequence is repeated. |



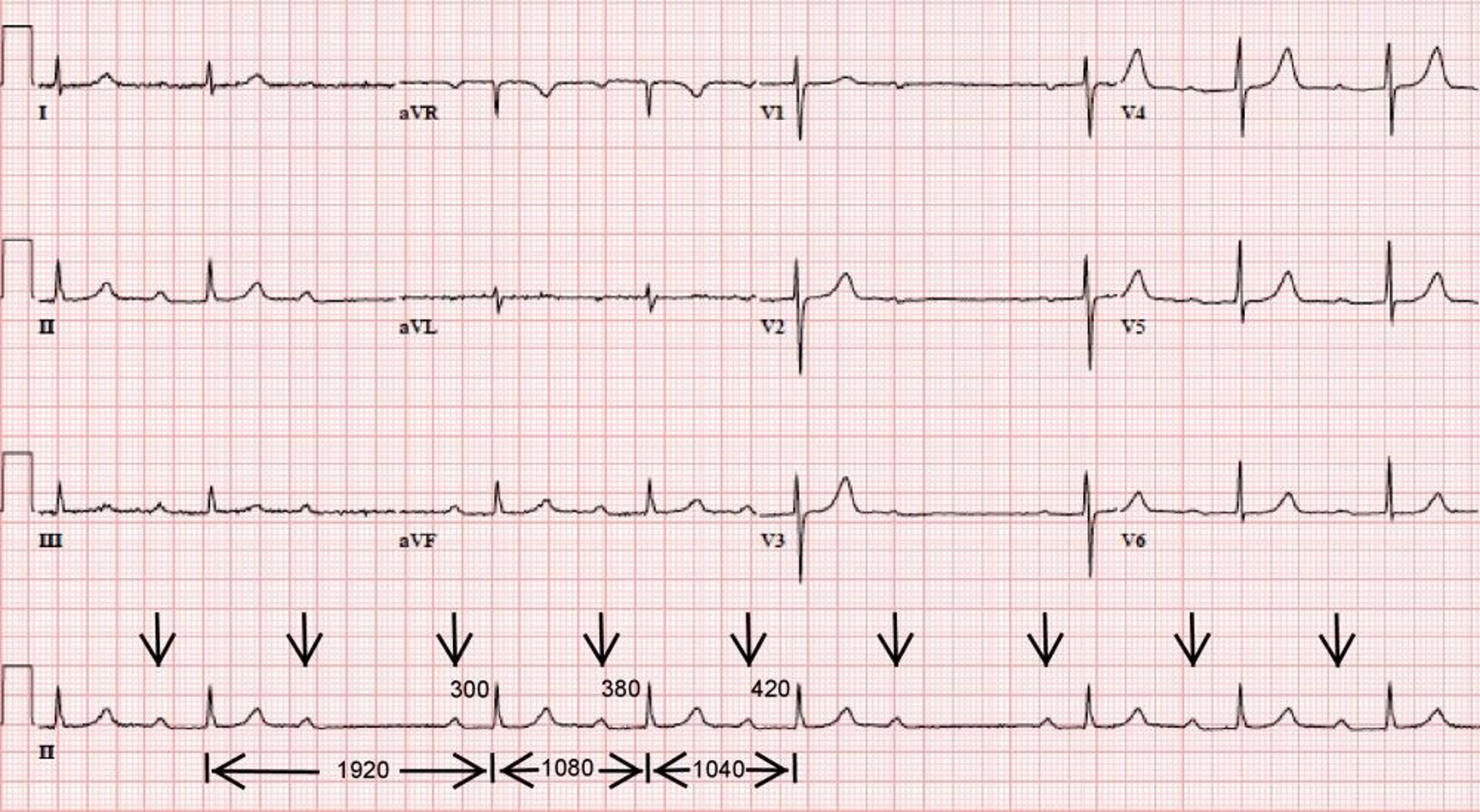
Image courtesy of L. Brent Mitchell, MD.
Mobitz type I second-degree AV block may be physiologic in younger and more athletic patients. If the QRS complex is narrow, Mobitz type I second-degree AV block is nearly always in the AV node; if the QRS complex is wide (> 0.12 second), Mobitz I second-degree AV block is more likely to be in the His-Purkinje system (60 to 70%) than in the AV node (30 to 40%) (2). AV nodal block usually progresses slowly, and if the block becomes complete, a reliable junctional escape rhythm at a reasonable rate (35 to 55 beats/minute) typically develops. Treatment is therefore often unnecessary unless the block causes symptomatic bradycardia and transient or reversible causes have been excluded. Treatment is pacemaker insertion, which may also benefit patients without symptoms who have Mobitz type I second-degree AV block at infranodal sites detected by electrophysiologic studies done for other reasons.
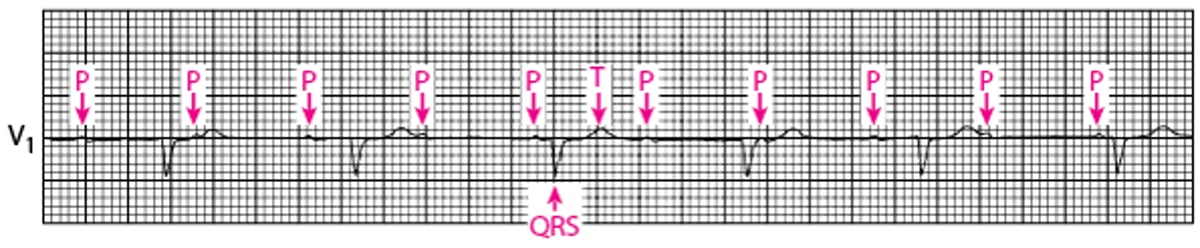
In Mobitz type II second-degree AV block, the PR interval remains constant. Beats are intermittently nonconducted and QRS complexes dropped, usually in a repeating cycle of every third (3:1 block) or fourth (4:1 block) P wave (see figure Mobitz Type II Second-Degree AV Block). The RR interval spanning the block is equal to twice the other RR intervals.
Mobitz Type II Second-Degree Atrioventricular Block
The PR interval remains constant. Beats are intermittently nonconducted, and QRS complexes dropped, usually in a repeating cycle of every third (3:1 block) or fourth (4:1 block) P wave. |


Mobitz type II second-degree AV block is always pathologic; the block occurs at the His bundle in 25% of patients and in the bundle branches in the rest (4). Patients may be asymptomatic or experience light-headedness, presyncope, and syncope, depending on the ratio of conducted to blocked beats. Progression of Mobitz type II second-degree AV block to complete heart block is typical and may be sudden, and the ventricular escape rhythm is both slower (20 to 40 beats/minute) than a junctional escape rhythm (35 to 50 beats/minute) and may be unreliable, giving way to asystole; therefore, in the absence of a transient or reversible cause, a pacemaker is indicated (3).
In high-grade second-degree AV block, every second (or more) P wave is blocked (see figure Second-Degree AV Block (High Grade)).
Second-Degree Atrioventricular Block (High Grade)
Every second P wave is blocked in this example of high-grade second-degree AV block. |


In patients with high-grade second-degree AV block, the distinction between Mobitz type I AV block and Mobitz type II AV block is difficult to make because 2 P waves are never conducted in a row. Risk of complete AV block is difficult to predict, and a pacemaker is usually indicated (5).
Patients with any form of second-degree AV block and a structural heart disorder should be considered candidates for permanent pacing unless there is a transient or reversible cause.
Third-degree AV block
In third-degree AV block, no P waves conduct to make QRS complexes. By definition, the P wave rate is greater than the QRS rate. Thus, heart block is complete in third-degree AV block (see figure Third-Degree AV Block).
Third-Degree Atrioventricular Block
There is no relationship between P waves and QRS complexes (AV dissociation) in third-degree AV block. The P wave rate is greater than the QRS rate. The underlying rhythm here is a junctional escape rhythm with narrow QRS complexes and a rate of approximately 65 beats/minute. |

There is no electrical communication between the atria and ventricles and thus no relationship between P waves and QRS complexes (AV dissociation). Cardiac function is maintained by an escape junctional or ventricular pacemaker. Escape rhythms originating above the bifurcation of the His bundle produce narrow QRS complexes, relatively rapid (35 to 50 beats/minute) and reliable heart rates, and mild symptoms (eg, fatigue, postural light-headedness, effort intolerance). Escape rhythms originating below the bifurcation produce wider QRS complexes, slower (20 to 40 beats/minute) and unreliable heart rates, and more severe symptoms (eg, presyncope, syncope, heart failure). Signs include those of AV dissociation, such as cannon a waves, blood pressure fluctuations, and variation in loudness of the first heart sound (S1). Risk of asystole-related syncope and sudden death is greater if low escape rhythms are present.
Most patients require a pacemaker. If the block is caused by antiarrhythmic medications, stopping the medication may be effective, although temporary pacing may be needed. However, even if the block reverses after stopping a negative dromotropic medication, block may later recur in the absence of the medication. Thus, ongoing surveillance is necessary. AV block caused by acute inferior myocardial infarction usually reflects atrioventricular nodal dysfunction due to increased parasympathetic tone and/or local adenosine release. It may respond to atropine or aminophylline and in most cases resolves spontaneously over several days. release. It may respond to atropine or aminophylline and in most cases resolves spontaneously over several days.
AV block caused by anterior myocardial infarction usually reflects extensive myocardial necrosis involving the His-Purkinje system and requires immediate transvenous pacemaker insertion with interim external pacing as necessary (5) Spontaneous resolution may occur but warrants evaluation of AV nodal and infranodal conduction (eg, electrophysiologic study, exercise testing, 24-hour ECG).
Most patients with isolated congenital third-degree AV block have a junctional escape rhythm that maintains a reasonable rate, but they require a permanent pacemaker before they reach middle age. Less commonly, patients with congenital AV block have a slow escape rhythm and require a permanent pacemaker at a young age, perhaps even during infancy.
References
1.Wogan JM, Lowenstein SR, Gordon GS: Second-degree atrioventricular block: Mobitz type II. J Emerg Med 11(1):47–54, 1993. doi:10.1016/0736-4679(93)90009-v
2. Nery PB, Beanlands RS, Nair GM, et al: Atrioventricular block as the initial manifestation of cardiac sarcoidosis in middle-aged adults. J Cardiovasc Electrophysiol 25(8):875–881, 2014. doi: 10.1111/jce.12401
3. Barold SS: Type I Wenckebach second-degree AV block: A matter of definition. Clin Cardiol 41(3):282–84, 2018. doi: 10.1002/clc.22874
4. Waller BF, Gering LE, Branyas NA, Slack JD: Anatomy, histology, and pathology of the cardiac conduction system--Part V. Clin Cardiol 16(7):565–569, 1993. doi:10.1002/clc.4960160710
5. Kusumoto FM, Schoenfeld MH, Barrett C, et al: 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm 16(9):e128–e226, 2019. doi: 10.1016/j.hrthm.2018.10.037
Key Points
There are 3 degrees of atrioventricular (AV) block: first, second, and third.
First-degree and second-degree blocks are partial and third-degree block is complete.
First-degree AV block is rarely symptomatic, and no treatment is required.
Second-degree AV block Mobitz type I may be physiologic and if heart rate slows, a reliable junctional escape rhythm typically develops and treatment is therefore unnecessary unless symptomatic bradycardia occurs.
Second-degree AV block Mobitz type II and third-degree AV block are always pathologic, and a pacemaker is typically required unless the cause is transient or reversible.







