


Lymphadenopathy is palpable enlargement of ≥ 1 lymph nodes. Diagnosis is clinical. Treatment is of the causative disorder.
(See also Overview of the Lymphatic System.)
Lymph nodes are present throughout the body and may be superficial or deep. Particular collections of superficial lymph nodes are present in the neck, axillae, and inguinal region; a few small (< 1 cm) nodes often are palpable in those areas in healthy people.
Lymphadenopathy is palpable enlargement (> 1 cm) of ≥ 1 lymph nodes; it is categorized as
Localized: When present in only 1 body area
Generalized: When present in ≥ 2 body areas
Lymphadenitis is lymphadenopathy with pain and/or signs of inflammation (eg, erythema [more subtle on dark skin], tenderness).
Other symptoms may be present depending on the underlying disorder.
Pathophysiology of Lymphadenopathy
Some plasma and cells (eg, cancer cells, infectious microorganisms) in the interstitial space, along with certain cellular material, antigens, and foreign particles enter lymphatic vessels, becoming lymphatic fluid. Lymph nodes filter the lymphatic fluid on its way to the central venous circulation, removing cells and other material. The filtering process also presents antigens to the lymphocytes contained within the nodes. The immune response from these lymphocytes involves cellular proliferation, which can cause the nodes to enlarge (reactive lymphadenopathy). Pathogenic microorganisms carried in the lymphatic fluid can directly infect the nodes, causing lymphadenitis, and cancer cells may lodge in and proliferate in the nodes.
Etiology of Lymphadenopathy
Because lymph nodes participate in the body's immune response, a large number of infectious and inflammatory disorders and cancers are potential causes (see table Some Causes of Lymphadenopathy). Only the more common causes are discussed here. Causes most likely vary depending on patient age, associated findings, and risk factors, but overall the most common causes are
Idiopathic, self-limited
Upper respiratory infections (URI)
Local soft-tissue infections
The most dangerous causes are
Cancer
Tuberculosis (TB)
However, most cases represent benign disorders or clinically obvious local infections. Approximately 1% of undifferentiated cases presenting for primary care involve cancer (1).
Some Causes of Lymphadenopathy
Cause | Suggestive Findings | Diagnostic Approach |
|---|---|---|
Cancers | ||
Leukemias (typically chronic and sometimes acute lymphocytic leukemia) | Fatigue, fever, weight loss, splenomegaly With acute leukemia, often easy bruising and/or bleeding | Complete blood count, peripheral smear, flow cytometry, bone marrow examination |
Painless adenopathy (local or generalized), often rubbery, sometimes matted Often fever, night sweats, weight loss, splenomegaly | Lymph node biopsy and flow cytometry | |
Metastatic cancers (often head and neck, thyroid, breast, or lung) | One or several painless local nodes Nodes often hard, sometimes fixed to adjacent tissue | Usually evaluation to identify the primary tumor Biopsy if primary cancer not found |
Systemic and systemic rheumatic disorders | ||
Tender cervical adenopathy in children Fever (usually > 39° C), truncal rash, strawberry tongue, periungual, palmar and plantar desquamation | Clinical criteria | |
Painless adenopathy (local or generalized) Often cough and/or dyspnea, fever, malaise, muscle weakness, weight loss, joint pains | Chest imaging (plain x-ray or CT) If imaging results are positive, node biopsy | |
Generalized adenopathy Typically arthritis or arthralgias Sometimes malar rash, other skin lesions | Clinical criteria Antibody testing | |
Other systemic rheumatic disorders (eg, juvenile idiopathic arthritis, Kikuchi lymphadenopathy (necrotizing histiocytic lymphadenitis), rheumatoid arthritis, Sjögren syndrome) | Vary | Varies |
Infections | ||
HIV infection (primary infection) | Generalized adenopathy Usually fever, malaise, rash, arthralgia Often history of HIV exposure or high-risk activity | HIV antibody testing Sometimes HIV-RNA assay (if early primary infection is suspected) |
Symmetric adenopathy, typically cervical but sometimes in axillae and/or inguinal areas Fever, sore throat, severe fatigue Often splenomegaly Typically in adolescents or young adults | Heterophile antibody test Sometimes Epstein-Barr virus serologic testing | |
Oropharyngeal infection (eg, pharyngitis, stomatitis, dental abscess) | Cervical adenopathy only (often tender) Clinically apparent oropharyngeal infection | Clinical evaluation |
Sexually transmitted infections (STIs—particularly herpes simplex, chlamydial infections, and syphilis) | Except for secondary syphilis, only inguinal adenopathy (fluctuant or draining nodes suggest lymphogranuloma venereum) Often urinary symptoms, urethral or cervical discharge Sometimes genital lesions For secondary syphilis, often widespread mucocutaneous lesions, generalized lymphadenopathy | For herpes simplex, culture For chlamydial infections, nucleic acid-based testing For syphilis, serologic testing |
Skin and soft-tissue infections (eg, cellulitis, abscess, cat-scratch disease), including direct lymph node infection | Usually a visible local lesion (or recent history of a lesion) distal to site of adenopathy Sometimes only erythema, tenderness of an isolated node (often cervical) without apparent primary site of entry | Usually clinical evaluation For cat scratch disease, serum antibody titers |
Bilateral, nontender cervical or axillary adenopathy Sometimes a flu-like syndrome, hepatosplenomegaly Often history of exposure to cat feces | Serologic testing | |
Tuberculosis (extrapulmonary tuberculosis—tuberculous lymphadenitis) | Usually cervical or supraclavicular adenopathy, sometimes inflamed or draining Often in patients with HIV infection | Tuberculin skin testing or interferon-gamma release assay Usually node aspiration or biopsy |
Upper respiratory infection | Cervical adenopathy with only little or no tenderness Sore throat, runny nose, cough | Clinical evaluation |
Other infections (eg, brucellosis, cytomegalovirus infection, histoplasmosis, paracoccidioidomycosis, plague, rat-bite fever, tularemia) | Vary Often risk factors (eg, geographic location, exposure) | Varies |
Other conditions | ||
History of using a causative medication Except for phenytoin, a serum sickness-type reaction (eg, rash, arthritis and/or arthralgias, myalgia, fever) | Clinical evaluation | |
Silicone breast implants | Localized adenopathy in patients with breast implants | Exclusion of other causes of adenopathy |
CT = computed tomography; HIV = human immunodeficiency virus. | ||
Etiology reference
1. Fijten GH, Blijham GH. Unexplained lymphadenopathy in family practice. An evaluation of the probability of malignant causes and the effectiveness of physicians' workup. J Fam Pract 1988;27(4):373-376. doi:10.1080/09503158808416945
Evaluation of Lymphadenopathy
Adenopathy may be the patient's reason for presenting or be discovered during evaluation for another complaint.
History
History of present illness should determine the location and duration of adenopathy and whether it is accompanied by pain. Recent cutaneous injuries (particularly cat scratches and rat bites) and infections in the area drained by affected nodes are noted.
Review of systems should seek symptoms of possible causes, including
Runny, congested nose (URI)
Sore throat (pharyngitis, mononucleosis)
Mouth, gum, or tooth pain (oral-dental infection)
Cough and/or dyspnea (sarcoidosis, lung cancer, TB, some fungal infections)
Fever, fatigue, and malaise (mononucleosis and many other infections, cancers, and systemic rheumatic disorders)
Genital lesions or discharge (herpes simplex, chlamydia, syphilis)
Joint pain and/or swelling (systemic lupus erythematosus [SLE] or other systemic rheumatic disorders)
Easy bleeding and/or bruising (leukemia)
Dry, irritated eyes (Sjögren syndrome)
Past medical history should identify risk factors for (or known) TB or HIV infection, and cancer (particularly use of alcohol and/or tobacco). Patients are queried about contacts who are ill (to assess risk of TB or viral illnesses, such as Epstein-Barr virus), sexual history (to assess risk of sexually transmitted infections), travel history to areas of endemic infections (eg, Middle East for brucellosis, American Southwest for plague) and possible exposures (eg, cat feces for toxoplasmosis, farm animals for brucellosis, wild animals for tularemia). Medication history is reviewed for specific known causative agents.
Physical examination
Vital signs are reviewed for fever. Areas of particular lymph node concentration in the neck (including occipital and supraclavicular areas), axillae, and inguinal region are palpated. Node size, tenderness, and consistency are noted as well as whether the nodes are freely mobile or fixed to adjacent tissue.

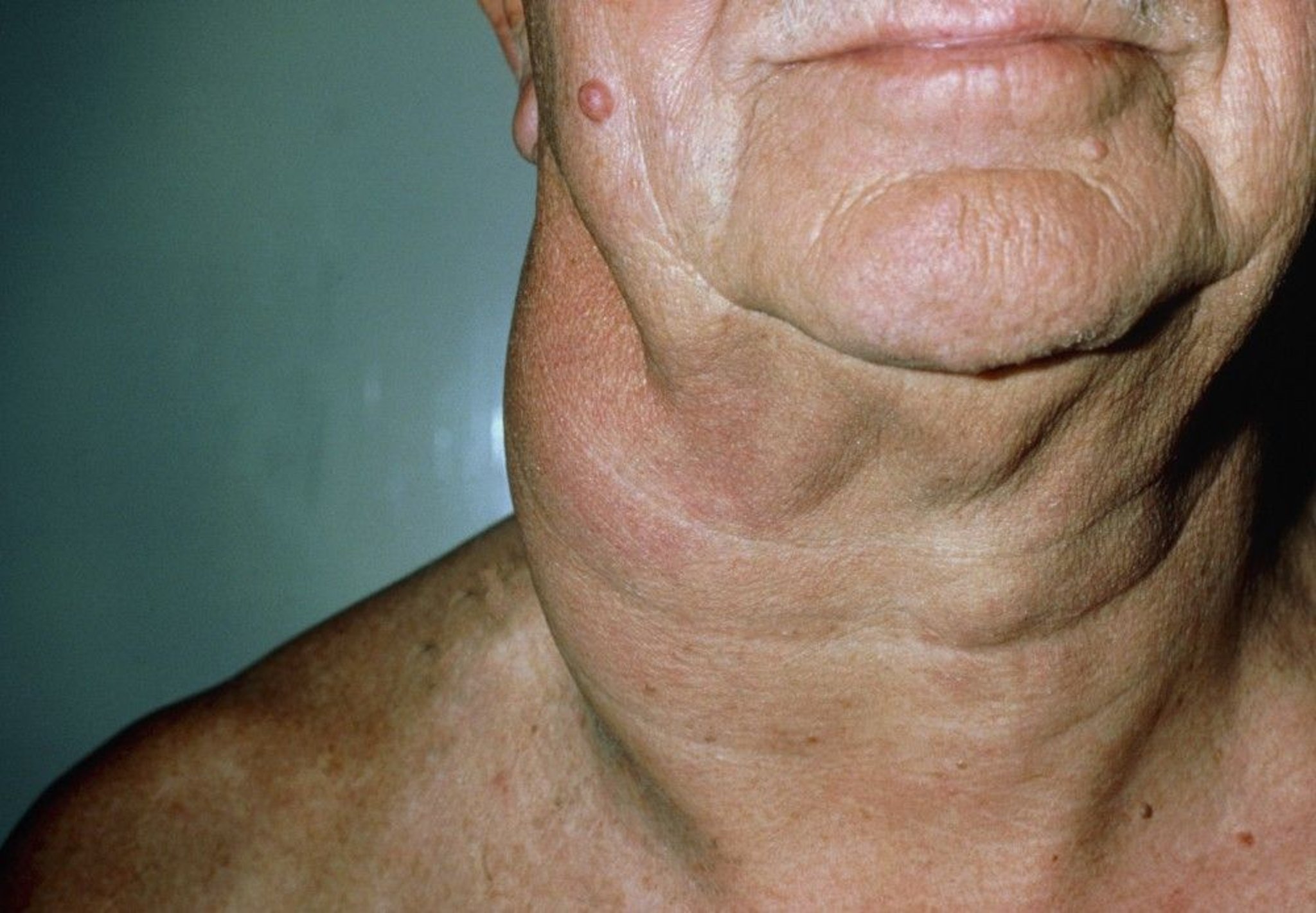
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
Skin is inspected for rash and lesions, with particular attention to areas drained by the affected nodes. The oropharynx is inspected and palpated for signs of infection and any lesions that may be cancerous. The thyroid gland is palpated for enlargement and nodularity. Breasts (including in males) are palpated for lumps. Lungs are auscultated for crackles (suggesting sarcoidosis or infection). Abdomen is palpated for hepatomegaly and splenomegaly. Genitals are examined for chancres, vesicles, and other lesions, and for urethral discharge. Joints are examined for signs of inflammation.
Red flags
Cervical or inguinal node > 2 cm or any palpable supraclavicular or axillary node regardless of size
Node that is draining, hard, or fixed to underlying tissue
Risk factors for HIV or TB
Fever and/or weight loss
Splenomegaly
Interpretation of findings
Patients with generalized adenopathy usually have a systemic disorder. However, patients with localized adenopathy may have a local or systemic disorder (including one that often causes generalized adenopathy).
Sometimes, history and physical examination suggest a cause (see table Some Causes of Lymphadenopathy) and may be diagnostic in patients with a clear viral upper respiratory infection or with local soft-tissue or dental infection. In other cases, findings (such as the red flag findings) are of concern but do not point to a single cause.
Cervical or inguinal nodes that are hard, markedly enlarged (> 2 cm—[1]), and/or fixed to adjacent tissue are concerning for cancer, particularly in patients who have had prolonged use of tobacco and/or alcohol. However, any palpable supraclavicular or axillary node not ascribable to infection regardless of size, should prompt concern about possible intrathoracic or breast cancer. Marked tenderness, erythema, and warmth in a single enlarged node may be due to a suppurative node infection (eg, due to staphylococcus or streptococcus).
Fever may occur with many of the infectious, malignant, and systemic rheumatic disorders. Splenomegaly can occur with mononucleosis, toxoplasmosis, leukemia, and lymphoma. Weight loss occurs with TB and cancer. Risk factors and travel and exposure history are at best suggestive.
Finally, adenopathy can have a serious cause in patients who have no other manifestations of illness.
Testing
If a specific disorder is suspected (eg, mononucleosis in a young patient with fever, sore throat, and splenomegaly), initial testing is directed at clinically indicated tests for that condition (see table Some Causes of Lymphadenopathy).
If history and physical examination do not show a likely cause, further evaluation depends on the nodes involved and the other findings present.
Patients with unexplained red flag findings and those with generalized adenopathy should have a complete blood count (CBC) and chest radiograph. If abnormal white blood cells are seen on CBC, a peripheral smear and flow cytometry are done to evaluate for leukemia or lymphoma. For generalized adenopathy, most clinicians usually also do a tuberculin skin test (or interferon-gamma release assay) and serologic tests for HIV, mononucleosis, and perhaps toxoplasmosis and syphilis. Patients with joint symptoms or rash should have antinuclear antibody testing for systemic lupus erythematosus.
Most clinicians believe patients with newly identified localized or generalized adenopathy and no other findings can safely be observed for 3 to 4 weeks, unless cancer is suspected. If cancer is suspected, patients typically require computed tomography (CT) or magnetic resonance imaging (MRI) of the area as clinically indicated and, depending on the findings, should have biopsy of the node and any abnormal tissue. Biopsy is also considered if isolated or generalized adenopathy does not resolve in 3 to 4 weeks (2).
Evaluation references
1. Slap GB, Brooks JS, Schwartz JS. When to perform biopsies of enlarged peripheral lymph nodes in young patients. JAMA 1984;252(10):1321-1326.
2. Bazemore AW, Smucker DR. Lymphadenopathy and malignancy. Am Fam Physician 2002;66(11):2103-2110.
Treatment of Lymphadenopathy
Primary treatment is directed at the cause; adenopathy itself is not treated.
A trial of corticosteroids is not done for adenopathy of unknown etiology because corticosteroids can reduce adenopathy caused by leukemia and lymphoma and thus delay diagnosis, and corticosteroids can exacerbate TB.
A trial of antibiotics is also not indicated, except when a suppurative lymph node infection is suspected.
Key Points
Most cases are idiopathic and self limited or result from clinically apparent local causes.
Initial testing should be done if there are red flag findings, if other manifestations or risk factors suggest a specific disorder, or when generalized adenopathy has no apparent cause.
Patients with newly identified localized or generalized lymphadenopathy and no other diagnostic findings can be observed for 3 to 4 weeks, after which time biopsy should be considered.







