



Abdominal aortic diameter ≥ 3 cm typically constitutes an abdominal aortic aneurysm. The cause is multifactorial, but atherosclerosis is often involved. Most aneurysms grow slowly (~10%/year) without causing symptoms, and most are found incidentally. Risk of rupture is proportional to the size of the aneurysm. Diagnosis is made by ultrasound or CT scanning. Treatment is surgery or endovascular stent grafting.

")
")
")

(See also Overview of Aortic Aneurysms.)
Abdominal aortic aneurysms (AAAs) account for three-fourths of aortic aneurysms and may affect between 0.4 and 7.6% of the population, depending on the population being studied (1). Prevalence is 3 times greater in males. AAAs typically begin below the renal arteries (infrarenal) (2) but may include the renal arterial ostia (pararenal); about 50% involve the iliac arteries. By definition, an aortic diameter ≥ 3 cm constitutes an AAA. Most AAAs are fusiform (circumferential widening of the artery). Many are lined with laminated thrombus.
General references
1. O'Donnell TFX, Landon BE, Schermerhorn ML. The case for expanding abdominal aortic aneurysm screening. J Vasc Surg 2020;71(5):1809-1812. doi:10.1016/j.jvs.2019.10.024
2. Jongkind V, Yeung KK, Akkersdijk GJ, et al. Juxtarenal aortic aneurysm repair. J Vasc Surg 2010;52(3):760-767. doi:10.1016/j.jvs.2010.01.049
Etiology of Abdominal Aortic Aneurysms
Etiology of abdominal aortic aneurysms is multifactorial but commonly involves a weakening of the arterial wall, usually by
Other causes include
Trauma
Cystic medial necrosis (degeneration of the aortic media)
Postsurgical anastomotic disruption
Vasculitis (eg, Takayasu arteritis)
Uncommonly, syphilis and localized bacterial or fungal infection, typically due to sepsis or infective endocarditis, weaken the arterial wall and cause infected (mycotic) aneurysms. Staphylococcus aureus is the number one cause of mycotic aneurysms, followed by Salmonella.
Risk factors
Risk factors for abdominal aortic aneurysms include
Smoking (strongest risk factor)
Older age (peak incidence at age 70 to 80 years)
Family history (in 15 to 25%)
Race (more common among White patients than among patients with African ancestry)
Male sex
Inherited connective tissue disorders (eg, Marfan syndrome, Ehlers-Danlos syndrome, Loeys-Dietz syndrome)
Symptoms and Signs of Abdominal Aortic Aneurysms
Most abdominal aortic aneurysms are asymptomatic. Symptoms and signs, when they do occur, may be nonspecific but usually result from compression of adjacent structures. As AAAs expand, they may cause pain, which is steady, deep, boring, visceral, and felt most prominently in the lumbosacral region. Patients may be aware of an abnormally prominent abdominal pulsation. Although most aneurysms grow slowly, rapidly enlarging aneurysms that are about to rupture can be tender.
The aneurysm may or may not be palpable as a pulsatile mass, depending on its size and patient habitus. The probability that a patient with a pulsatile palpable mass has a small aneurysm (ie, < 4 cm) is about 55% (positive predictive value); the probability exceeds 80% only when the mass is > 5 cm in diameter (1). A systolic bruit may be audible over the aneurysm.
Patients with an occult AAA sometimes present with symptoms of complications or of the cause (eg, fever, malaise, or weight loss due to infection or vasculitis).
Complications
The main complications of abdominal aortic aneurysms include
Rupture
Distal embolization
Disseminated intravascular coagulation (uncommon)
Rupture is most likely to occur on the left posterolateral wall 2 to 4 cm below the renal arteries. If an AAA ruptures, most patients die before reaching a medical facility. Patients who do not die immediately typically present with abdominal or back pain, hypotension, and tachycardia. They may have a history of recent upper abdominal trauma, often minimal, or isometric straining (eg, lifting a heavy object). Even patients who reach the hospital alive have about a 50% mortality (2).
Distal embolization of thrombus or atheromatous material may dislodge and block arteries of the kidneys, bowel, and lower extremities. When a lower extremity artery is blocked, patients typically present with sudden unilateral extremity pain and often pallor and loss of pulses (see also Acute Peripheral Arterial Occlusion).
Uncommonly, large AAAs cause disseminated intravascular coagulation, perhaps because large areas of abnormal endothelial surface trigger rapid thrombosis and consumption of coagulation factors.
Symptoms and signs references
1. Venkatasubramaniam AK, Mehta T, Chetter IC, et al. The value of abdominal examination in the diagnosis of abdominal aortic aneurysm. Eur J Vasc Endovasc Surg 2004;27(1):56-60. doi:10.1016/j.ejvs.2003.09.006
2. Durieux R, Lardinois MJ, Albert A, Defraigne JO, Sakalihasan N. Outcomes and Predictors of Mortality in a Belgian Population of Patients Admitted with Ruptured Abdominal Aortic Aneurysm and Treated by Open Repair in the Contemporary Era. Ann Vasc Surg 2022;78:197-208. doi:10.1016/j.avsg.2021.05.015
Diagnosis of Abdominal Aortic Aneurysms
Often an incidental finding on physical examination or a radiologic study
Confirmation by ultrasound or abdominal CT scanning
Sometimes CT angiography or magnetic resonance angiography
Most abdominal aortic aneurysms are diagnosed incidentally when they are detected during physical examination or when abdominal ultrasound, CT, or MRI is done for other reasons. An AAA should be considered in older patients who present with acute abdominal pain or back pain whether a palpable pulsatile mass is present or not.

This patient has an abdominal aortic aneurysm measuring 3.4 cm (between the white crosses) as well as atherosclerotic plaque or mural thrombus (red arrow).
© 2017 Elliot K. Fishman, MD.

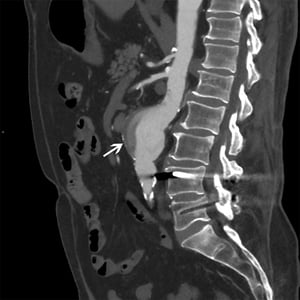
The white arrow shows an abdominal aortic aneurysm measuring 5 cm with heterogenous flow and mural plaque.
© 2017 Elliot K. Fishman, MD.

The white arrow shows a suprarenal abdominal aortic pseudoaneurysm. There is also extensive plaque in the infrarenal aorta and iliac arteries.
© 2017 Elliot K. Fishman, MD.
This patient has an abdominal aortic aneurysm measuring 3.4 cm (between the white crosses) as well as atherosclerotic plaque or mural thrombus (red arrow).
© 2017 Elliot K. Fishman, MD.
The white arrow shows an abdominal aortic aneurysm measuring 5 cm with heterogenous flow and mural plaque.
© 2017 Elliot K. Fishman, MD.
The white arrow shows a suprarenal abdominal aortic pseudoaneurysm. There is also extensive plaque in the infrarenal aorta and iliac arteries.
© 2017 Elliot K. Fishman, MD.
When symptoms or physical examination findings suggest AAA, ultrasound, CT, or MRI of the abdomen are usually the tests of choice (1). Patients with symptoms should have immediate testing to make the diagnosis before catastrophic rupture. For patients who are hemodynamically unstable with presumed rupture, ultrasound provides bedside results more rapidly, but intestinal gas and distention may limit its accuracy.
Laboratory tests, including a complete blood count (CBC), electrolytes, blood urea nitrogen (BUN), creatinine, prothrombin time (PT), partial thromboplastin time (PTT), and blood type and cross-match, are done in preparation for possible surgery.
If rupture is not suspected, CT angiography (CTA) or magnetic resonance angiography (MRA) can more precisely characterize aneurysm size and anatomy. If thrombi line the aneurysm wall, conventional angiography may underestimate true size; CT may provide a more accurate estimate. Aortography is sometimes necessary if renal artery or aortoiliac disease is suspected or if correction with endovascular stent grafts (endografts) is being considered.
Plain abdominal radiographs are neither sensitive nor specific; however, if obtained for other purposes, radiographs may show aortic calcification outlining the aneurysm wall.
If a mycotic aneurysm is suspected, bacterial and fungal blood cultures should be done.
Screening males age > 65 years who have ever smoked with abdominal ultrasound decreases mortality, but the absolute reduction is small for males who are otherwise at low risk. Screening also can also provoke anxiety, particularly for aneurysms managed expectantly. Some authorities recommend shared decision-making.
Diagnosis reference
1. Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation 2022;146(24):e334-e482. doi:10.1161/CIR.0000000000001106
Treatment of Abdominal Aortic Aneurysms
Medical management, particularly smoking cessation and blood pressure control
Surgery or endovascular stent grafting
Some abdominal aortic aneurysms enlarge at a rate of 10%/year. Enlargement often occurs in a stepwise pattern with periods of no growth observed. Other aneurysms enlarge exponentially.
Control of atherosclerotic risk factors, especially smoking cessation and use of antihypertensive medications as appropriate, is important. If a small (< 4 cm) or moderate-sized (between 4 and 5 cm) aneurysm. When the aneurysm becomes > 5 cm in a female or > 5.5 cm in a male and if risk of perioperative complications is lower than estimated risk of rupture, AAA repair is indicated (1). Risk of rupture versus that of perioperative complications should be discussed frankly with the patient.
The need for surgical treatment is related to aneurysm size, which is linked to the risk of rupture (see table Abdominal Aortic Aneurysm Size and Rupture Risk).
Abdominal Aortic Aneurysm Size and Rupture Risk*
AAA Diameter | Rupture Risk (%/year) |
|---|---|
< 4 cm | 0 |
4–4.9 cm | 0.5–5% |
5–5.9 cm* | 3–15% |
6–6.9 cm | 10–20% |
7–7.9 cm | 20–40% |
> 8 cm | 30–50% |
* Elective surgical repair should be considered for aneurysms > 5.0–5.5 cm. | |
AAA = abdominal aortic aneurysm. | |
Data from Brewster DC, Cronenwett JL, Hallett JW Jr, et al. Guidelines for the treatment of abdominal aortic aneurysms. Report of a subcommittee of the Joint Council of the American Association for Vascular Surgery and Society for Vascular Surgery. J Vasc Surg 2003;37(5):1106-1117. doi:10.1067/mva.2003.363 | |
Ruptured abdominal aortic aneurysms require immediate open surgery or endovascular stent grafting. Without treatment, mortality rate approaches 100%. There is no clear difference in mortality for open surgical treatment compared with endovascular stent grafting (2). Mortality remains high because many patients have coexisting coronary, cerebrovascular, and peripheral atherosclerosis.
Patients who present in hemorrhagic shock require fluid resuscitation and blood transfusions, but mean arterial pressure should not be elevated to > 70 to 80 mm Hg (permissive hypotension) because bleeding may increase. Preoperative blood pressure control and avoidance of hypertension are important.

Pearls & Pitfalls
|
Elective surgical repair is recommended for
Aneurysms > 5 cm in females and > 5.5 cm in males (when risk of rupture increases to > 5 to 10%/year), unless coexisting medical conditions contraindicate surgery (1)
Additional indications for elective surgery include
Increase in aneurysm size by > 0.5 cm within 6 months, regardless of size
Chronic abdominal pain
Thromboembolic complications
Iliac or femoral artery aneurysm that causes lower-limb ischemia
Aneurysms > 4.5 cm in patients with Marfan syndrome
Before elective repair, clinical consideration of coronary artery disease (CAD) is often needed and may or may not require further evaluation (see table Tests for Assessing Cardiac Anatomy and Function) because some patients with an AAA have significant risk of cardiovascular events. Aggressive medical treatment and risk factor control are essential. Routine preoperative coronary angioplasty or bypass surgery has not been shown to be necessary in most patients who can be prepared with good medical management before aneurysm repair; coronary revascularization should be considered only in patients with unstable coronary artery disease (eg, acute coronary syndrome, including unstable angina) or multiple risk factors for coronary artery disease.
Surgical repair consists of replacing the aneurysmal portion of the abdominal aorta with a synthetic graft. If the iliac arteries are involved, the graft must be extended to include them. If an aorto-bifemoral repair is done, it is important to ensure flow to at least one internal iliac artery (hypogastric artery) to avoid vasculogenic erectile dysfunction and pelvic ischemia. If the aneurysm extends above the renal arteries, the renal arteries must be reimplanted into the graft, or bypass grafts must be created.
Placement of an endovascular stent graft within the aneurysmal lumen via the femoral artery is a less invasive alternative that has a lower acute morbidity and mortality than open repair. This procedure excludes the aneurysm from systemic blood flow and reduces risk of rupture. The aneurysm eventually thromboses, and 50% of aneurysms decrease in diameter. Short-term results are good, and long-term results are favorable (3). Complications include angulation, kinking, thrombosis, migration of the stent graft, and endoleak (persistent flow of blood into the aneurysm sac after endovascular stent graft placement). Thus, follow-up visits must be more frequent after endovascular stent graft placement than after a surgical repair. If no complications occur, imaging tests are recommended at 1 month, 6 months, 12 months, and every year thereafter. Complex anatomy (eg, short aneurysm neck below renal arteries, severe arterial tortuosity) makes routine endovascular stent grafting difficult in these patients; however, devices have been developed to overcome these issues. In general, for a successful endovascular repair, surgeons should choose a specific device that is appropriate for the patient's anatomic characteristics.
In most cases, repair of aneurysms < 5 cm does not appear to increase survival. Aneurysms should be monitored with ultrasound or abdominal CT scans every 6 to 12 months for expansion that warrants treatment.
Treatment of a mycotic aneurysm consists of vigorous antimicrobial therapy directed at the pathogen, followed by excision of the aneurysm. Early diagnosis and treatment improve outcome.
Surgical complications
Myocardial infarction is the leading cause of early postoperative death.
Complications following abdominal aortic aneurysm repair include
Major vein injury due to proximal cross clamping
Erectile dysfunction (as a result of nerve damage or decreased blood flow)
Graft infection
Pseudoaneurysm
Atherosclerotic occlusion of graft
Treatment references
1. Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation 2022;146(24):e334-e482. doi:10.1161/CIR.0000000000001106
2. Badger S, Forster R, Blair PH, Ellis P, Kee F, Harkin DW. Endovascular treatment for ruptured abdominal aortic aneurysm. Cochrane Database Syst Rev. 2017;5(5):CD005261. Published 2017 May 26. doi:10.1002/14651858.CD005261.pub4
3. EVAR trial participants. Endovascular aneurysm repair versus open repair in patients with abdominal aortic aneurysm (EVAR trial 1): randomised controlled trial. Lancet 2005;365(9478):2179-2186. doi:10.1016/S0140-6736(05)66627-5
Key Points
Abdominal aortic diameter ≥ 3 cm constitutes an abdominal aortic aneurysm (AAA).
AAAs typically enlarge at a rate of 10%/year, but some enlarge exponentially; about 20% remain the same size indefinitely.
Risk of rupture is proportional to the size of the aneurysm.
Diagnose using ultrasound or abdominal CT; for unruptured aneurysms, CT angiography or magnetic resonance angiography can more precisely characterize aneurysm size and anatomy.
Ruptured AAAs require immediate open surgery or endovascular stent grafting; even then, mortality is high.
Elective surgical repair is recommended for aneurysms > 5 cm in females, for those > 5.5 cm in males, and for those that are rapidly enlarging or causing ischemic or embolic complications.







