


Glaucomas are a group of eye disorders characterized by progressive optic nerve damage (often, but not always, associated with increased eye pressure) that can lead to irreversible loss of vision.
Damage to the optic nerve can occur when pressure within the eye increases.
Usually, the vision loss occurs so slowly that it may not be noticed for a long time.
People at risk should have a complete eye examination, including measurement of eye pressures and testing of side (peripheral) vision.
Eye pressure needs to be controlled throughout life, usually with eye drops but sometimes with eye surgery.
Almost 3 million people in the United States and 64 million people worldwide have glaucoma. Glaucoma is the second most common cause of blindness worldwide and the second most common cause of blindness in the United States, where it is the leading cause of blindness among Black and Hispanic people. Only half of the people who have glaucoma know they do. Glaucoma can occur at any age but is 6 times more common among people over age 60.
People at highest risk are those with any of the following:
Age older than 40
Black race
Family members who have (or had) the disease
Nearsightedness (in open-angle glaucoma) or farsightedness (in closed-angle glaucoma)
Long-term use of corticosteroids
Previous eye injury or surgery
Glaucoma occurs when an imbalance in production and drainage of fluid in the eye (aqueous humor) increases eye pressure to unhealthy levels. Normally the aqueous fluid, which nourishes the eye, is produced by the ciliary body behind the iris (in the posterior chamber) and flows through the pupil to the front of the eye (anterior chamber), where it exits into drainage canals between the iris and cornea (the “angle”). When functioning properly, the system works like a faucet (ciliary body) and a drain in a sink (drainage canals). Balance between fluid production and drainage—between an open faucet and a properly draining sink—keeps the fluid flowing freely and prevents pressure in the eye from building up.
Normal Fluid Drainage
Fluid is produced in the ciliary body behind the iris (in the posterior chamber), passes into the front of the eye (anterior chamber), and then exits through the drainage canals or the uveoscleral pathway (black arrows). |

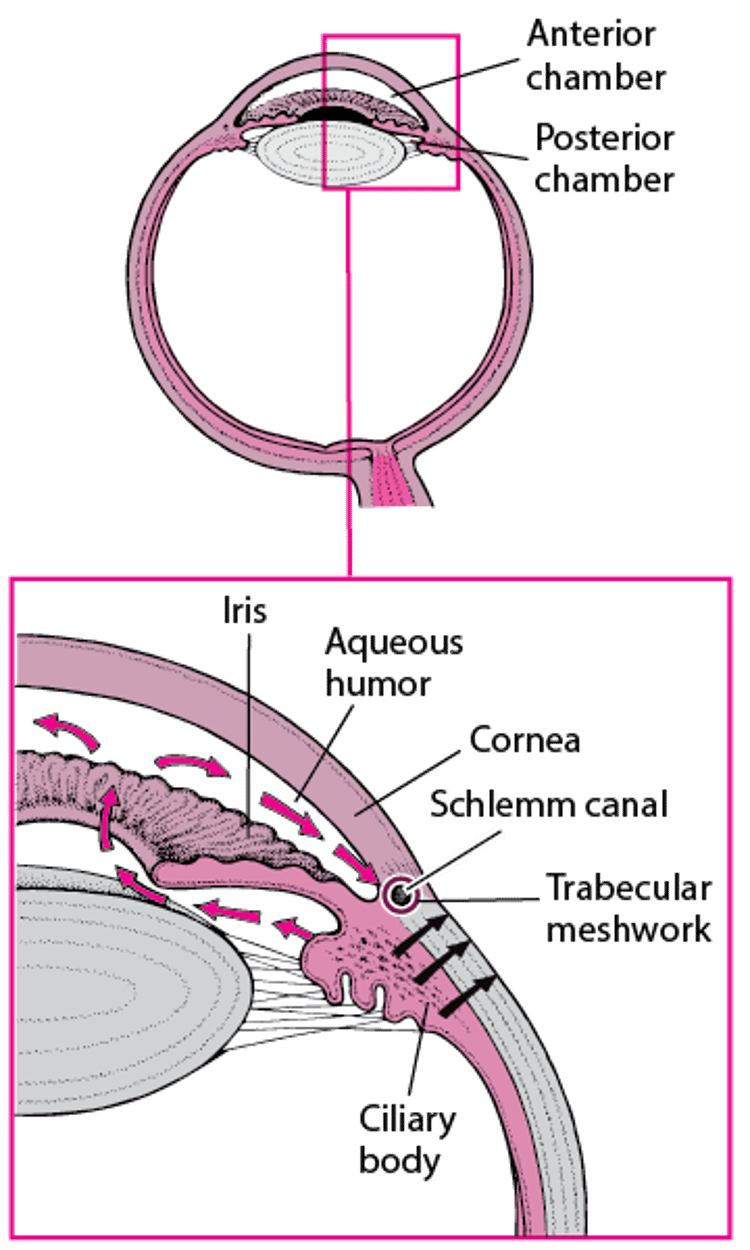
In glaucoma, the drainage canals become clogged, blocked, or covered. Fluid cannot leave the eye even though new fluid is being produced in the posterior chamber. In other words, the sink “backs up” while the faucet is still running. Because there is nowhere in the eye for the fluid to go, pressure in the eye increases. When the pressure becomes higher than the optic nerve can tolerate, damage to the optic nerve occurs. This damage causes glaucoma.
Sometimes eye pressure increases within the range of normal but is nonetheless too high for the optic nerve to tolerate (called low-tension glaucoma or normal-tension glaucoma). In the United States, about one third of people who have glaucoma have low-tension glaucoma. Low-tension glaucoma is more common among Asian people.
In most people, the cause of glaucoma is not known. When the cause of glaucoma is not known, it is called primary glaucoma. When the cause of glaucoma is known, it is called secondary glaucoma. Causes of secondary glaucoma include certain medications, infection, inflammation, tumors, large cataracts or other conditions, and surgery for cataracts. These causes keep the fluid from draining freely, which leads to increased eye pressure and optic nerve damage.
Types of glaucoma
There are many forms of adult and childhood glaucomas. Most glaucomas fall into two categories:
Open-angle glaucoma
Closed-angle glaucoma (angle-closure glaucoma)
Open-angle glaucoma is more common than closed-angle glaucoma. In open-angle glaucoma, the drainage canals in the eyes gradually become clogged with tiny, microscopic deposits over months or years. This type of glaucoma is "open" because the canals are not visibly blocked (when examined under magnification, as with a slit lamp), but drainage through them is still inadequate. Pressure in the eye rises slowly because fluid is produced at a normal rate but drains sluggishly.
Closed-angle glaucoma is less common than open-angle glaucoma. In closed-angle glaucoma, the drainage canals in the eyes become blocked or covered because the angle between the iris and cornea is too narrow. This type of glaucoma is "closed" because the canals are visibly blocked. The blockage can occur suddenly (called acute closed-angle glaucoma) or slowly (called chronic closed-angle glaucoma). If the blockage occurs suddenly, pressure in the eye rises rapidly. If the blockage occurs slowly, the pressure in the eye rises slowly as in open-angle glaucoma.
Symptoms of Glaucoma
Open-angle glaucoma
Open-angle glaucoma is painless and causes no early symptoms. Both eyes usually are affected but typically not equally. The main symptom of open-angle glaucoma is the development of blind spots, or patches of vision loss, over months to years. The blind spots slowly grow larger and merge together. Peripheral vision is usually lost first. People may miss stairs, notice portions of words missing when reading, or have difficulty with driving. Vision loss occurs so gradually that it is often not noticed until much of it is lost. Because central vision is generally lost last, many people develop tunnel vision: they see straight ahead perfectly but become blind in all other directions. If glaucoma is left untreated, eventually even tunnel vision is lost, and a person becomes totally blind.
Closed-angle glaucoma
In acute closed-angle glaucoma, eye pressure rises rapidly, and people typically notice severe eye pain and headache, redness, blurred vision, rainbow-colored halos around lights, and sudden loss of vision. They may also have nausea and vomiting as a response to the increase in eye pressure. Acute closed-angle glaucoma is considered a medical emergency because people can lose their vision as quickly as 2 to 3 hours after the appearance of symptoms if the condition is not treated.
In chronic closed-angle glaucoma, eye pressure rises slowly, and symptoms usually begin as in open-angle glaucoma. Some people may have eye redness, discomfort, blurred vision, or a headache that lessens with sleep. The eye pressure may be normal but usually is higher in the affected eye.
People who have had open-angle glaucoma or closed-angle glaucoma in one eye are likely to develop it in the other.
Diagnosis of Glaucoma
A doctor's examination of the eyes
If doctors suspect glaucoma (for example, based on what they find during a routine eye examination), they do a comprehensive eye examination for glaucoma. There are five parts to a comprehensive eye examination for glaucoma:
Measurement of eye pressure
Evaluation of the optic nerve
Visual field testing
Gonioscopy
Measurement of the corneas
Doctors measure pressure in the eye. This measurement is taken painlessly with an instrument called a tonometer. Normal eye pressure readings are in the range of 11 to 21 millimeters of mercury (mm Hg). In general, eye pressure readings greater than 21 mm Hg are considered high.
But measuring eye pressure is not enough because a third or more of people with glaucoma have eye pressure in the average range, and some people have a high eye pressure reading that is not caused by glaucoma. So doctors also use an ophthalmoscope and sometimes other instruments (such as optical coherence tomography) to look for changes in the optic nerve that indicate damage caused by glaucoma.
In addition, visual field testing (peripheral vision testing) allows a doctor to detect blind spots. Most often, visual field testing is done with a machine that determines the person’s ability to see small dots of light in all areas of the visual field.
Doctors may also use a special lens to examine the drainage channels in the eye, a procedure known as gonioscopy. The gonioscope allows the doctor to determine whether the glaucoma is of the open-angle or closed-angle type.
Doctors also measure the thickness of the corneas. If the corneas are thin, glaucoma is more likely to develop. However, a thin cornea does not mean that glaucoma is present.
Did You Know...
|
Screening
Because the most common types of glaucoma can cause slow and silent loss of vision over years, early detection of the disease is extremely important. All people at high risk of glaucoma (see the list of risk factors) should have a routine comprehensive eye examination every 1 to 2 years.
Treatment of Glaucoma
Medications
Sometimes surgery
Once a person loses vision because of glaucoma, the loss is permanent. But if glaucoma is detected, proper treatment can prevent further vision loss. So the goal of glaucoma treatment is to prevent further optic nerve damage and vision loss by lowering the pressure in the eye.
Treatment of glaucoma is lifelong. It involves decreasing eye pressure by increasing fluid drainage out of the eyeball or by reducing the amount of fluid produced inside the eyeball. Some people with high eye pressure who do not have signs of optic nerve damage (known as glaucoma “suspects”) can be monitored closely without treatment.
Medications, usually in the form of eye drops, and surgery are the main treatments for glaucoma. The type and severity of glaucoma determine the appropriate treatment:
Most people with open-angle glaucoma respond well to the medications used for treatment.
These medications are also used for people with closed-angle glaucoma, but surgery, not eye drops, is the main treatment.
Medications
Glaucoma eye drops are typically safe but they may cause a variety of side effects. People need to use them for the rest of their lives, and regular checkups are necessary to monitor eye pressure, optic nerves, and visual fields. Typically, the medications are used in only one eye (called a one-eye trial) at first or both eyes. If there is improvement in the treated eye after 1 to 4 weeks, both eyes are treated.
Acute closed-angle glaucoma
Medications Used to Treat Glaucoma
Medication | Some Side Effects | Comments |
|---|---|---|
Prostaglandin-like compounds | ||
Increased eye and skin pigmentation Elongated and thickened eyelashes Muscle, joint, and back pain Rash Possible worsening of inflammation within the front part of the eye (uveitis) | How they work: Increase aqueous humor outflow Given as: Eye drops Other comments: These drops have few serious bodywide side effects. | |
Beta-blockers | ||
Levobetaxalol | Shortness of breath in people with asthma or other lung disorders that cause wheezing Slow heart beat Insomnia Fatigue Depression Confusion Sexual dysfunction See table Antihypertensive Medications | How they work: Decrease aqueous humor production Given as: Eye drops Other comments: These drops do not affect pupil size. Some side effects are worse in people with heart or blood vessel disease. Some side effects may develop slowly and may be mistakenly attributed to aging or other bodily processes. |
Cholinergic medications* | ||
Sweating Headache Involuntary, shaking movement Tremor Excess saliva production Diarrhea, abdominal cramps, nausea | How they work: Constrict the pupil (miosis) and increase aqueous humor outflow Given as: Eye drops Other comments: These drops are not as effective as beta-blockers. People who have darker pupils may need high-strength drops. These medications make it harder for the eyes to adapt to darkness. | |
Cholinesterase inhibitors* | ||
Same as for cholinergic agonists but more likely to occur | How they work: Constrict the pupil (miosis) and increase aqueous humor outflow Given as: Eye drops Other comments: These drops are very long acting. They can cause cataracts and retinal detachment and should not be taken by people who have closed-angle glaucoma. These medications make it harder for the eyes to adapt to darkness. | |
Rho kinase inhibitor | ||
Eye redness Broken blood vessels in the eye Corneal deposits | How they work: Increase aqueous humor outflow Given as: Eye drops | |
Alpha-adrenergic agonists | ||
Increase in blood pressure or heart rate Abnormal heart rhythm May excessively dilate the pupil High rate of allergic reactions and decreased response if given over a period of time so that larger doses are required to have the same effect (tachyphylaxis) May cause dry mouth, has a lower rate of allergic reactions than the other medications, and can be fatal in children less than 2 years of age | How they work: Decrease aqueous humor production and increase aqueous humor outflow Given as: Eye drops | |
Carbonic anhydrase inhibitors | ||
Fatigue Altered taste Loss of appetite Depression Kidney stones Body salt (electrolyte) abnormalities Numbness or tingling Low or high blood cell counts (blood dyscrasias) Weight loss Nausea Diarrhea Bad taste in the mouth Rash | How they work: Decrease aqueous humor production Given as: | |
Osmotic diuretics | ||
Increase urine production Can have serious side effects in some people (for example, worsening of heart failure or brain dysfunction) by changing body salt (electrolyte) levels or may cause dehydration | How they work: Increase concentration of salts in the blood, which draws fluid from the eye by osmosis Given as: Other comments: These medications are used most often to treat acute closed-angle glaucoma. | |
* These medications are rarely used. | ||
Surgery
Surgery may be needed for people whose eye pressure is extremely high, whose eye pressure is not effectively controlled by eye drops, who cannot take eye drops, who develop intolerable side effects from the eye drops, or who already have severe visual field damage when they initially see a doctor.
Laser surgery can be used to increase drainage (laser trabeculoplasty) in people with open-angle glaucoma or to make an opening in the iris (laser peripheral iridotomy) in people with acute or chronic closed-angle glaucoma. Laser surgery is done in the doctor’s office or in a hospital or clinic. Anesthetic eye drops are used to prevent pain. People are usually able to go home the day of the procedure. Evidence suggests that treatment with laser surgery is at least as effective as medical therapy in open-angle glaucoma. It is acceptable and often advisable to initiate treatment with laser trabeculeculoplasty for newly people newly diagnosed.
The most common complication of glaucoma laser surgery is a temporary increase in eye pressure, which is treated with glaucoma eye drops. Rarely, the laser used in laser surgery may burn the cornea, but these burns usually heal quickly.
Glaucoma filtration surgery is the other form of surgery doctors use to treat glaucoma. With traditional glaucoma filtration surgery, doctors manually create a new drainage system (trabeculectomy or tube shunt) to allow fluid to bypass the clogged or blocked canals and filter out of the eye. Traditional glaucoma filtration surgery is typically done in a hospital. People can usually go home the same day.
Partial thickness procedures (viscocanalostomy, deep sclerectomy, and canaloplasty) are alternative filtration procedures that are used to remove only part of the drainage system to enhance the outflow of fluid. These procedures may be done in a hospital or in an outpatient surgery center. People can usually go home the same day.
The trabeculectomy filtration procedure can rarely cause severe infection in the eye (endophthalmitis). Glaucoma filtration surgery may cause acceleration of cataract growth, eye pressures that are too low, or swelling in the back of the eye.
Secondary glaucoma
The treatment of glaucoma caused by other disorders depends on the cause.
For infection or inflammation, antibiotic, antiviral, or corticosteroid eye drops may provide a cure.
A tumor that blocks fluid drainage should be treated, as should a cataract that is so large it causes eye pressure to rise. Removing such a cataract can help prevent secondary glaucoma but occasionally increases eye pressure. High eye pressure that results from cataract surgery is treated with glaucoma eye drops that reduce eye pressure. If eye drops do not work, glaucoma filtration surgery can be done.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
The Glaucoma Research Foundation: Access to information on innovative research to find a cure for glaucoma as well as basic information on care and treatment of people with the condition.
American Council of the Blind (ACB): Programs and services to enhance the quality of life for blind and visually impaired people, including Braille forums and publications, ACB Radio programs, and other relevant media.
American Foundation for the Blind: Access to research, educational, and employment initiatives to expand opportunities for people with blindness or visual impairment.




