


Acute viral hepatitis is diffuse liver inflammation caused by specific hepatotropic viruses that have diverse modes of transmission and epidemiologies. Although acute viral hepatitis can be asymptomatic, a nonspecific viral prodrome is often followed by anorexia, nausea, and often fever or right upper quadrant pain. Jaundice can develop, typically as other symptoms begin to resolve. Most cases resolve spontaneously, but some progress to chronic hepatitis. Occasionally, acute viral hepatitis progresses to acute liver failure (indicating fulminant hepatitis). Diagnosis is by liver tests and serologic tests to identify the virus. Good hygiene and universal precautions can prevent acute viral hepatitis. Depending on the specific virus, preexposure and postexposure prophylaxis may be possible using vaccines or serum globulins. Treatment is usually supportive.
(See also Causes of Hepatitis and Neonatal Hepatitis B Virus Infection.)
Acute viral hepatitis is a common, worldwide disease that has different causes; each type shares clinical, biochemical, and morphologic features. The term acute viral hepatitis often refers to infection of the liver by one of the hepatitis viruses. Other viruses (eg, Epstein-Barr virus, yellow fever virus, cytomegalovirus) can also cause acute viral hepatitis but less commonly.
Etiology of Acute Viral Hepatitis
At least 5 specific viruses appear to be responsible (see table Characteristics of Hepatitis Viruses) for acute viral hepatitis:
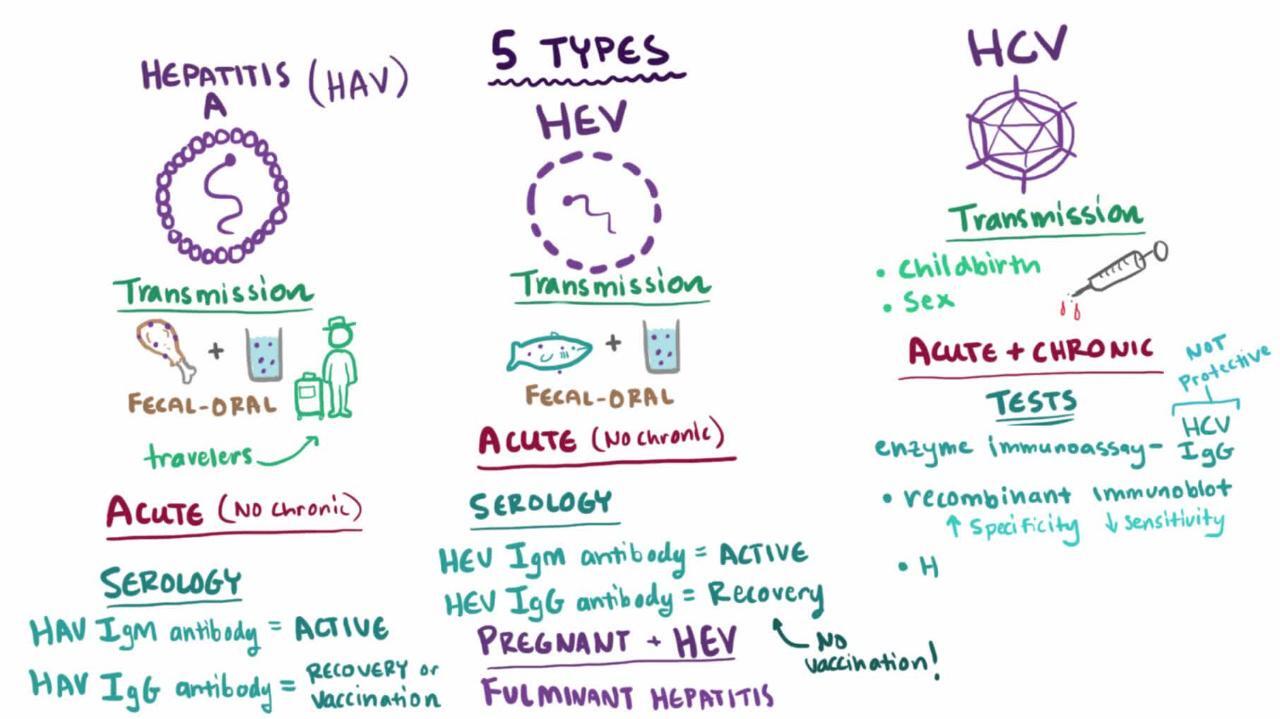
Hepatitis A (HAV)
Hepatitis B (HBV)
Hepatitis C (HCV)
Hepatitis D (HDV)
Hepatitis E (HEV)
Other unidentified viruses probably also cause acute viral hepatitis.
Characteristics of Hepatitis Viruses
Characteristic | Hepatitis A Virus | Hepatitis B Virus | Hepatitis C Virus | Hepatitis D Virus | Hepatitis E Virus |
|---|---|---|---|---|---|
Nucleic acid | RNA | DNA | RNA | * | RNA |
Serologic diagnosis | IgM anti-HAV | HBsAg | Anti-HCV | Anti-HDV | Anti-HEV |
Major transmission | Fecal-oral | Blood | Blood | Needle | Water |
Incubation period (days) | 15–45 | 40–180 | 20–120 | 30–180 | 14–60 |
Epidemics | Yes | No | No | No | Yes |
Chronicity | No | Yes | Yes | Yes | No |
Liver cancer | No | Yes | Yes | Yes | No |
* Incomplete RNA; requires presence of hepatitis B virus for replication. | |||||
Anti-HCV = antibody to hepatitis C virus; anti-HDV = antibody to hepatitis D virus; anti-HEV = antibody to hepatitis E virus; HBsAg = hepatitis B surface antigen; IgM anti-HAV = IgM antibody to hepatitis A virus. | |||||
Symptoms and Signs of Acute Viral Hepatitis
Some manifestations of acute hepatitis are virus-specific (see discussions of individual hepatitis viruses) and some patients are asymptomatic, but in general, acute infection tends to develop in predictable phases:
Incubation period: The virus multiplies and spreads without causing symptoms (see table Characteristics of Hepatitis Viruses).
Prodromal (pre-icteric) phase: Nonspecific symptoms occur; they include profound anorexia, malaise, nausea and vomiting, a newly developed distaste for cigarettes (in smokers), and often fever or right upper quadrant abdominal pain. Urticaria and arthralgias occasionally occur, especially in HBV infection.
Icteric phase: After 3 to 10 days, the urine darkens, followed by jaundice. Systemic symptoms often regress, and patients feel better despite worsening jaundice. The liver is usually enlarged and tender, but the edge of the liver remains soft and smooth. Mild splenomegaly occurs in 15 to 20% of patients. Jaundice usually peaks within 1 to 2 weeks.
Recovery phase: During this 2- to 4-week period, jaundice fades.
Appetite usually returns after the first week of symptoms. Acute viral hepatitis usually resolves spontaneously 4 to 8 weeks after symptom onset.
Anicteric hepatitis (hepatitis without jaundice) occurs more often than icteric hepatitis in patients with HCV infection and in children with HAV infection. It typically manifests as a minor flu-like illness.
Recrudescent hepatitis occurs in a few patients and is characterized by recurrent manifestations during the recovery phase.
Manifestations of cholestasis may develop during the icteric phase (called cholestatic hepatitis) but usually resolve. When they persist, they cause prolonged jaundice, elevated alkaline phosphatase, and pruritus, despite general regression of inflammation.
Diagnosis of Acute Viral Hepatitis
Liver tests (aspartate aminotransferase [AST] and alanine aminotransferase [ALT] elevated out of proportion to alkaline phosphatase, usually with hyperbilirubinemia)
Viral serologic testing
Prothrombin/international normalized ratio (PT/INR) measurement
Initial diagnosis of acute hepatitis
Acute hepatitis must first be differentiated from other disorders that cause similar symptoms. In the prodromal phase, hepatitis mimics various nonspecific viral illnesses and is difficult to diagnose. Anicteric patients suspected of having hepatitis based on risk factors are tested initially with liver tests, including aminotransferases, bilirubin, and alkaline phosphatase. Acute hepatitis often manifests in the icteric phase and so should be differentiated from other disorders causing jaundice (see figure Simplified Diagnostic Approach to Possible Acute Viral Hepatitis).
Acute hepatitis can usually be differentiated from other causes of jaundice by
Its marked elevations of AST and ALT: Often ≥ 400 IU/L (6.68 microkat/L)
ALT is typically higher than AST, but absolute levels correlate poorly with clinical severity. Values increase early in the prodromal phase, peak before jaundice is maximal, and fall slowly during the recovery phase. Urinary bilirubin usually precedes jaundice. Hyperbilirubinemia in acute hepatitis varies in severity, and fractionation has no clinical value. Alkaline phosphatase is usually only moderately elevated; marked elevation suggests extrahepatic cholestasis and prompts imaging tests (eg, ultrasonography).
Liver biopsy is usually not needed unless the diagnosis is uncertain.
If laboratory results suggest acute hepatitis, particularly if ALT and AST are > 1000 IU/L (16.7 microkat/L), PT/INR is measured to assess liver function.
Manifestations of portosystemic encephalopathy combined with bleeding diathesis or prolongation of INR suggest acute liver failure, indicating fulminant hepatitis.
If acute hepatitis is suspected, efforts are next directed toward identifying its cause. A history of exposure may provide the only clue of drug-induced or toxic hepatitis. The history should also elicit risk factors for viral hepatitis.
Prodromal sore throat and diffuse adenopathy suggest infectious mononucleosis rather than viral hepatitis.
Simplified Diagnostic Approach to Possible Acute Viral Hepatitis
* Obtain additional laboratory studies for hepatitis A (see table Hepatitis A Serology), hepatitis B (see table Hepatitis B Serology), and hepatitis C (see table Hepatitis C Serology). ALT = alanine aminotransferase; anti-HCV = antibody to hepatitis C virus; AST = aspartate aminotransferase; HBsAg = hepatitis B surface antigen; IgM anti-HAV = IgM antibody to hepatitis A virus. |


Serology
In patients with findings suggesting acute viral hepatitis, the following studies are done to screen for hepatitis viruses A, B, and C:
IgM antibody to HAV (IgM anti-HAV)
Hepatitis B surface antigen (HBsAg)
IgM antibody to hepatitis B core (IgM anti-HBc)
Antibody to HCV (anti-HCV)
Hepatitis C RNA (HCV-RNA) polymerase chain reaction
If any are positive, further serologic testing may be necessary to differentiate acute from past or chronic infection (see tables Hepatitis A Serology, Hepatitis B Serology, and Hepatitis C Serology).
If serologically confirmed HBV infection is severe, anti-HDV is measured.
If the patient has recently traveled to an endemic area or is immunosuppressed, IgM antibody to HEV (IgM anti-HEV) should be measured if the test is available.
Biopsy
Biopsy is usually unnecessary but, if done, usually reveals similar histopathology regardless of the specific virus:
Patchy cell dropout
Acidophilic hepatocellular necrosis
Mononuclear inflammatory infiltrate
Histologic evidence of regeneration
Preservation of the reticulin framework
HBV infection can occasionally be diagnosed based on the presence of ground-glass hepatocytes (caused by HBsAg-packed cytoplasm) and using special immunologic stains for the viral components. However, these findings are unusual in acute HBV infection and are much more common in chronic HBV infection.
Treatment of Acute Viral Hepatitis
Supportive care
Treatment of acute hepatitis C, partly to prevent transmission to others
No treatments attenuate acute viral hepatitis. Alcohol should be avoided because it can increase liver damage. Restrictions on diet or activity, including commonly prescribed bed rest, have no scientific basis.
Patients with acute HCV infection should be treated with antiviral therapy upon initial diagnosis without awaiting spontaneous resolution in order to prevent transmission to others. Owing to the high efficacy and safety, the same regimens that are recommended for chronic HCV infection are recommended for acute infection (1).
Viral hepatitis should be reported to the local or state health department.
Treatment reference
1. American Association for the Study of Liver Diseases (AASLD) and Infection Diseases Society of America (IDSA): HCV Guidance: Recommendations for Testing, Managing, and Treating Hepatitis C. Management of Acute HCV Infection. Accessed May 7, 2024.
Prevention of Acute Viral Hepatitis
Because treatments have limited efficacy, prevention of viral hepatitis is very important.
General measures
Good personal hygiene helps prevent transmission, particularly fecal-oral transmission as occurs with HAV and HEV.
Blood and other body fluids (eg, saliva, semen) of patients with acute HBV and HCV infection and stool of patients with HAV infection are considered infectious. Barrier protection is recommended, but isolation of patients does little to prevent spread of HAV and is of no value in HBV or HCV infection.
Posttransfusion infection is minimized by avoiding unnecessary transfusions and by screening all donors for hepatitis B and C. Screening has decreased the incidence of posttransfusion hepatitis B and hepatitis C, which are now extremely rare in the United States.
Immunoprophylaxis
Immunoprophylaxis can involve active immunization using vaccines and passive immunization.
Vaccines for hepatitis A and hepatitis B are available in the United States.
Routine vaccination for hepatitis A and B is recommended in the United States for all children and for adults at high risk (see Adult Immunization Schedule).
A vaccine for hepatitis E is not available in the United States but is available in China.
No product exists for immunoprophylaxis of HCV or HDV. However, prevention of HBV infection prevents HDV infection. The propensity of HCV for changing its genome hampers vaccine development.
Key Points
Transmission is the fecal-oral route for hepatitis A and E parenterally or via blood for hepatitis B and C.
Hepatitis B and C, unlike hepatitis A, predispose to chronic hepatitis and liver cancer (if chronic).
Patients with acute viral hepatitis may be anicteric or even asymptomatic.
Do viral serologic testing (IgM anti-HAV, HBsAg, anti-HCV) if clinical findings are consistent with acute viral hepatitis and AST and ALT are elevated out of proportion to alkaline phosphatase.
Treat patients supportively. Treat acute hepatitis C to prevent transmission.
Routine vaccination for hepatitis A and B is recommended in the United States for all children and for adults at high risk.







