


Developmental dysplasia of the hip (formerly congenital dislocation of the hip) is abnormal development of the hip joint.
(See also Introduction to Congenital Craniofacial and Musculoskeletal Disorders.)
Developmental dysplasia of the hip leads to subluxation or dislocation; it can be unilateral or bilateral. High risk factors include
Presence of other deformities (eg, torticollis, congenital foot deformity)
Positive family history (particularly for girls)
Developmental dysplasia of the hip seems to result from laxity of the ligaments around the joint or from in utero positioning. Asymmetric skin creases in the thigh and groin are common, but such creases also occur in infants without developmental dysplasia of the hip. If the dysplasia remains undetected and untreated, the affected leg eventually becomes shorter, and the hip may become painful. Abduction of the hip is often impaired due to adductor spasm.
All infants are screened by physical examination. Because physical examination has limited sensitivity, high-risk infants and those with abnormalities found during physical examination typically should have an imaging study.
Two screening maneuvers commonly are used:
Ortolani maneuver: Detects the hip sliding back into the acetabulum
Barlow maneuver: Detects the hip sliding out of the acetabulum
Each hip is examined separately. Both maneuvers begin with the infant supine and the hips and knees flexed to 90° (the feet will be off the bed).
To do the Ortolani maneuver, the thigh of the hip being tested is abducted (ie, the knee is moved away from the midline into a frog-leg position) and gently pulled anteriorly. Instability is indicated by the palpable, sometimes audible, clunk of the femoral head moving over the posterior rim of the acetabulum and relocating in the cavity.
Next, in the Barlow maneuver, the hip is returned to the starting position and then slightly adducted (ie, the knee is drawn across the body) and the thigh is pushed posteriorly. A clunk indicates that the head of the femur is moving out of the acetabulum.
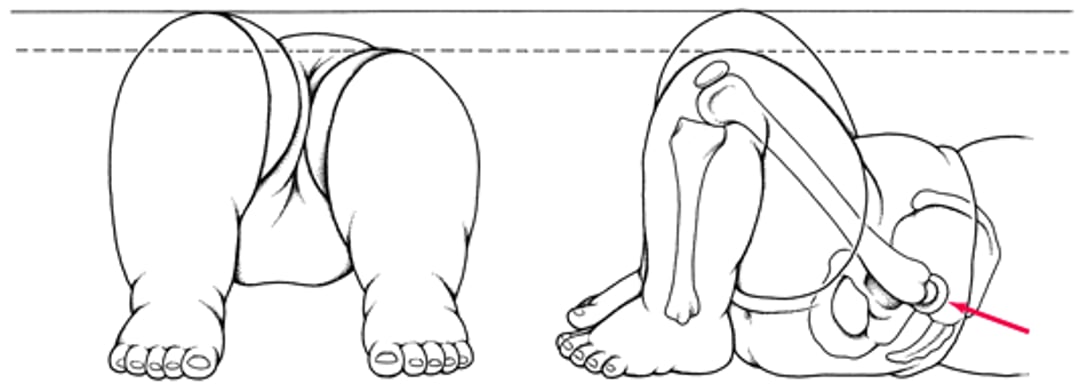
Also, a difference in knee height when the child is supine with hips flexed, knees bent, and feet on the examining table (Galeazzi sign, see figure) suggests dysplasia, especially unilateral. Somewhat later (eg, by 3 or 4 months of age), subluxation or dislocation is indicated by inability to completely abduct the thigh when the hip and knee are flexed; abduction is impeded by adductor spasm, which is often present even if the hip is not actually dislocated at the time of examination. Minor benign clicks are commonly detected. Although clicks usually disappear within 1 or 2 months, they should be checked regularly. Because bilateral dysplasia may be difficult to detect at birth, periodic testing for limited hip abduction during the first year of life is advised.
Galeazzi sign
The child is positioned as shown. The knee is lower on the affected side because of posterior displacement in the developmentally dysplastic hip (arrow). |

Ultrasonography of the hips is recommended at 6 weeks of age for infants at high risk, including those with a breech presentation, those born with other deformities (eg, torticollis, congenital foot deformity), and girls with a positive family history of developmental dysplasia of the hip.
Imaging is also required when any abnormality is suspected during examination. Hip ultrasonography can accurately establish the diagnosis earlier in life. Hip x-rays are helpful after the bones have started to ossify, typically after age 4 months.
Early treatment of the dysplasia is critical. With any delay, the potential for correction without surgery decreases steadily. The hip usually can be reduced immediately after birth, and with growth, the acetabulum can form a nearly normal joint. Treatment is with devices, most commonly the Pavlik harness, which hold the affected hips abducted and externally rotated. The Frejka pillow and other splints may help. Padded diapers and double or triple diapering are not effective and should not be done to correct developmental dysplasia of the hip.







