


Deformities are often considered together with dystrophies, but the two are slightly different; deformities are generally considered to be gross changes in nail shape, whereas dystrophies are changes in nail texture or composition (eg, onychomycosis).
About 50% of nail dystrophies result from fungal infection. The remainder result from various causes, including trauma, congenital abnormalities, psoriasis, lichen planus, benign tumors, and occasionally cancer.
Onychomycosis as a cause of nail dystrophy may be obvious on examination, but often samples of the nail plate and subungual debris are taken and sent for histopathologic examination and periodic acid-Schiff (PAS) examination, culture, or, more recently, polymerase chain reaction (PCR) analysis (1, 2).
Nonfungal dystrophies may require a tissue biopsy of the nail plate or nail matrix to make a diagnosis. Nail dystrophy may resolve with treatment of the cause, but, if not, manicurists may be able to mask nail changes with appropriate trimming and polishes.
(See also Overview of Nail Disorders.)
General references
1. Hafirassou AZ, Valero C, Gassem N, et al: Usefulness of techniques based on real time PCR for the identification of onychomycosis-causing species. Mycoses 60(10):638–644, 2017. doi: 10.1111/myc.12629
2. Gupta AK, Nakrieko KA: Onychomycosis infections: Do polymerase chain reaction and culture reports agree? J Am Podiatr Med Assoc 107(4):280–286, 2017. doi: 10.7547/15-136
Congenital nail deformities
In some congenital ectodermal dysplasias, patients have no nails (anonychia). In pachyonychia congenita, the nail beds are thickened, discolored, and transversely hypercurved (pincer nail deformity). Nail-patella syndrome causes triangular lunulae and partially absent thumb nails. Patients with Darier disease can have nails with red and white streaks and a distal V-shaped nick.


Nail deformities and dystrophies associated with systemic problems
In Plummer-Vinson syndrome (esophageal webs caused by severe, untreated iron deficiency), 50% of patients have koilonychia (concave, spoon-shaped nails).
Yellow nail syndrome is a rare condition characterized by slow-growing, thickened, hypercurved, yellow nails. This condition typically occurs in patients with lymphedema and/or chronic respiratory disorders. Chronic bronchial infections are present in about half of reported cases.
Half-and-half nails (Lindsay nails) occur usually with renal failure; the proximal half of the nail is white, and the distal half is pink or red-brown. Half-and-half nails occur in 20 to 50% of patients who have chronic kidney disease; however, this nail abnormality has been reported in various other chronic diseases including Crohn disease, cirrhosis, pellagra, and Kawasaki disease. This abnormality also occurs in healthy people (1).
Terry nails are characterized by whiteness of about 80% of the nail bed with a 0.5- to 3.0-mm brown-to-pink distal band. Terry nails are often associated with cirrhosis, chronic heart failure, and adult-onset diabetes mellitus. Differentiation from half-and-half nails can be difficult (1).
White nails occur with cirrhosis, although the distal third may remain pinker. Intensely white nails, also called Terry nails, can be present in patients with chronic liver or kidney failure, heart failure, or diabetes. Terry nails are a type of leukonychia; the abnormality is not in the nail itself but rather the nail bed, causing the nail the appear white. In Terry nails, nearly the entire nail is opaque white and the lunula is not visible. There is a thin zone of normal pink nail bed at the distal edge of the nail. Terry nails may sometimes occur as part of normal aging (1).
Beau lines are horizontal grooves in the nail plate that occur when nail growth temporarily slows, which can occur after infection, trauma, systemic illness, or during cycles of chemotherapy. Onychomadesis similarly results from temporary growth arrest of the nail matrix and differs from Beau lines in that the full thickness of the nail is involved, causing a proximal separation of the nail plate from the nail bed. Onychomadesis most frequently occurs several months after hand-foot-and-mouth disease but can occur after other viral infections. Nails affected by Beau lines or onychomadesis regrow normally with time.


Characteristic spoon-shaped (concave) nail of a patient with iron-deficiency anemia.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY


This image shows yellow nails with increased thickening and hypercurvature characteristic of yellow nail syndrome.
© Springer Science+Business Media


In this image of Terry nails, almost all of the nail is opaque white except for a narrow brown-to-pink band at the distal edge of the nail.
© Springer Science+Business Media


This image shows Beau lines in a patient undergoing multiple cycles of chemotherapy. Each line corresponds to a cycle of treatment.
© Springer Science+Business Media

The transverse depression of the nail plate is easily appreciated looking at the nail from the side.
© Springer Science+Business Media
Characteristic spoon-shaped (concave) nail of a patient with iron-deficiency anemia.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
This image shows yellow nails with increased thickening and hypercurvature characteristic of yellow nail syndrome.
© Springer Science+Business Media
In this image of Terry nails, almost all of the nail is opaque white except for a narrow brown-to-pink band at the distal edge of the nail.
© Springer Science+Business Media
This image shows Beau lines in a patient undergoing multiple cycles of chemotherapy. Each line corresponds to a cycle of treatment.
© Springer Science+Business Media
The transverse depression of the nail plate is easily appreciated looking at the nail from the side.
© Springer Science+Business Media
Systemic nail deformities and dystrophies reference
1. Pitukweerakul S, Pilla S: Terry's nails and Lindsay's nails: Two nail abnormalities in chronic systemic diseases. J Gen Intern Med 31(8):970, 2016. doi: 10.1007/s11606-016-3628-z
Nail deformities associated with dermatologic conditions
In psoriasis, nails may have a number of changes, including irregular pits, oil spots (localized areas of tan-brown discoloration), separation of part of the nail from the nail bed (onycholysis), and thickening and crumbling of the nail plate. Nail psoriasis is independently associated with treatment-resistant psoriatic disease and is a risk factor for development of psoriatic arthritis. Treatment of nail psoriasis is challenging, but immunomodulatory agents are the most effective (1, 2). Topical therapies can lead to modest improvement. Device-based therapies (eg, laser, light) need more study to judge their effectiveness.
Lichen planus of the nail matrix initially causes potentially reversible nail changes, including longitudinal ridging, fissuring, erythema of the lunula, and distal splitting of the nail. Over time, scarring and irreversible changes may occur, including nail atrophy, pterygium formation, and total nail loss. Lichen planus of the nail unit requires management early in the disease to prevent permanent disfigurement. Treatment options include topical, intralesional, and systemic corticosteroids. However, relapse may occur after therapy in some patients. Pterygium of the nail, which is caused by lichen planus, is characterized by scarring from the proximal nail outward in a V formation, which leads ultimately to nail loss.


This photo shows irregular pits and areas of yellow-brown discoloration (oil spots) in a person with psoriasis.
© Springer Science+Business Media


Nail bed psoriasis causes onycholysis (as evidenced by the white discoloration of the distal nails with erythematous border and absence of distal nail on the ring and little fingers). The underlying nail bed is hyperkeratotic.
© Springer Science+Business Media


The photo on the left shows thickening and crumbling of the nail of the great toe. Pitting and onycholysis are visible on the hand (right), suggesting nail psoriasis as the diagnosis.
© Springer Science+Business Media


This photo shows longitudinal ridging of the thumbnail of a patient with lichen planus of the nail.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY


This photo shows dorsal pterygium of several nails accompanied by atrophy of the nails.
© Springer Science+Business Media
This photo shows irregular pits and areas of yellow-brown discoloration (oil spots) in a person with psoriasis.
© Springer Science+Business Media
Nail bed psoriasis causes onycholysis (as evidenced by the white discoloration of the distal nails with erythematous border and absence of distal nail on the ring and little fingers). The underlying nail bed is hyperkeratotic.
© Springer Science+Business Media
The photo on the left shows thickening and crumbling of the nail of the great toe. Pitting and onycholysis are visible on the hand (right), suggesting nail psoriasis as the diagnosis.
© Springer Science+Business Media
This photo shows longitudinal ridging of the thumbnail of a patient with lichen planus of the nail.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
This photo shows dorsal pterygium of several nails accompanied by atrophy of the nails.
© Springer Science+Business Media
Dermatologic nail deformities references
1. van de Kerkhof P, Guenther L, Gottlieb AB, et alJ Eur Acad Dermatol Venereol 31(3):477–482, 2017. doi: 10.1111/jdv.14033
2. Merola JF, Elewski B, Tatulych S, et al:J Am Acad Dermatol 77(1):79–87, 2017. doi: 10.1016/j.jaad.2017.01.053
Discoloration
Cancer chemotherapy drugs (especially the taxanes) can cause melanonychia (nail plate pigmentation), which can be diffuse or may occur in transverse bands. Some drugs can cause characteristic changes in nail coloration:
Quinacrine: Nails appear greenish yellow or white under ultraviolet light.
Arsenic: Nails may turn diffusely brown.
Gold therapy: Nails may be light or dark brown.
Silver salts (argyria): Nails may be diffusely blue-gray.
Tobacco smoking or nail polish can result in yellow or brownish discoloration of nails and fingertips.


Image provided by Thomas Habif, MD.
White transverse lines of the nails (Mees lines) may occur with chemotherapy, acute arsenic intoxication, malignant tumors, myocardial infarction, thallium and antimony intoxication, fluorosis, and even during etretinate therapy. These lines are not due to changes in the nail bed, but are a true leukonychia, and the nails can grow out normally if the insulting exposure has been removed. Mees lines also develop with trauma to the finger, although traumatic white lines usually do not span the entire nail.


The fungus Trichophyton mentagrophytes causes a chalky white discoloration of the surface of the nail plate.
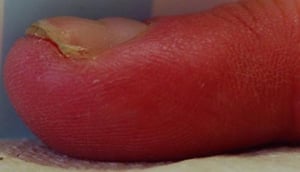
Green-nail syndrome is caused by infection with Pseudomonas. It is generally a harmless infection, usually of 1 or 2 nails, and is noteworthy for its striking blue-green color. It often occurs in patients with onycholysis or chronic paronychia whose nails have been exposed to irritants or have had excessive exposure to water. If the onycholysis or chronic paronychia is treated effectively, the Pseudomonas infection will resolve. Alternatively, topical gentamycin ointment can be effective in chronic cases. Patients should avoid irritants and excess moisture. Frequent clipping of the nail increases the response to treatment.


Median nail dystrophy (median canaliform dystrophy)


Melanonychia striata
Melanonychia striata are hyperpigmented bands that are longitudinal and extend from the proximal nail fold and cuticle to the free distal end of the nail plate. Pigmentation results from deposition of melanin by melanocytes in the nail matrix. Deposition of melanin is increased by melanocyte activation (increased production of melanin in the nail cells) or by melanocytic hyperplasia (increased production of melanocytes in the nail matrix).

Melanocytic hyperplasia can be caused by benign conditions, such as nail matrix melanocytic nevus or nail lentigo, or by malignant melanoma. Factors more often associated with malignant melanoma of the nail matrix include new onset after middle age, presence of pigmentation on the dominant thumb or hallux, rapid growth or darkening, bandwidth > 3 mm, associated nail plate dystrophy, or Hutchinson sign (extension of hyperpigmentation onto the proximal and/or lateral nail fold). Rapid biopsy and treatment are essential in cases of suspected melanoma (1).


Melanonychia striata reference
1. Leung AKC, Lam JM, Leong KF, Sergi CM: Melanonychia striata: Clarifying behind the black curtain. A review on clinical evaluation and management of the 21st century. Int J Dermatol 58(11):1239–1245, 2019. doi: 10.1111/ijd.14464
Onycholysis
Irritant contact dermatitis of the hands and fingers may lead to onycholysis (1). Colonization of the nail bed with Candida albicans may occur, but treating the underlying irritant exposure leads to resolution of the onycholysis, with or without treating the Candida.
Partial onycholysis may also occur in patients with psoriasis or thyrotoxicosis.


Onycholysis reference
1. Vélez NF, Jellinek NJ: Simple onycholysis: A diagnosis of exclusion. J Am Acad Dermatol 70(4):793–794, 2014. doi: 10.1016/j.jaad.2013.09.061
Pincer nail deformity
Pincer nail deformity is a transverse over-curvature of the nail plate. It is most often caused by onychomycosis, psoriasis, tumors of the nail apparatus, and poorly fitting shoes. It has also been reported in patients with systemic lupus erythematosus, Kawasaki disease, end-stage renal disease, and some genetic syndromes (eg, paronychia congenita). Patients often have pain at the borders of the nail where the nail plate curves into the tips of the fingers or toes. There is no established treatment of choice, but a number of surgical techniques have been successful (1, 2, 3).


Pincer nail deformity references
1. Demirkıran ND: Suture treatment for pincer nail deformity: An inexpensive and simple technique. Dermatol Surg 46(4):573–576, 2019. doi: 10.1097/DSS.0000000000001818
2. Shin WJ, Chang BK, Shim JW, et al: Nail plate and bed reconstruction for pincer nail deformity. Clin Orthop Surg 10(3):385–388, 2018. doi: 10.4055/cios.2018.10.3.385
3. Won JH, Chun JS, Park YH, et al: Treatment of pincer nail deformity using dental correction principles. J Am Acad Dermatol 78(5):1002–1004, 2018. doi: 10.1016/j.jaad.2017.08.014
Trachyonychia
Trachyonychia (rough, opaque nails) may occur with alopecia areata, lichen planus, atopic dermatitis, and psoriasis. It is most common among children. When present in all nails, trachyonychia is often called 20-nail dystrophy. When it occurs in children, it tends to resolve spontaneously. When it occurs in adults, treatment is aimed at the underlying disorder.


Nail tumors
Benign and malignant tumors can affect the nail unit, causing deformity. Benign tumors include myxoid cysts, pyogenic granulomas, and glomus tumors. Malignant tumors include Bowen disease, squamous cell carcinoma, and malignant melanoma. When cancer is suspected, expeditious biopsy followed by referral to a surgeon is strongly advised.


DR P. MARAZZI/SCIENCE PHOTO LIBRARY







