



- Overview of Fractures
- Growth Plate Fractures
- Collarbone Fractures
- Upper Arm Fractures
- Elbow Fractures
- Middle Forearm Fractures
- Wrist Fractures
- Hand Fractures
- Fractures of the Palm
- Finger Fractures
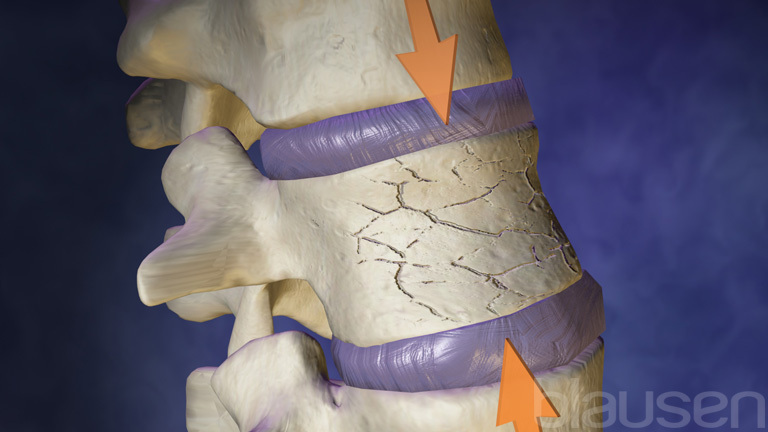
- Compression Fractures of the Spine
- Pelvic Fractures
- Hip Fractures
- Leg Fractures
- Ankle Fractures
- Fractures of the Heel Bone
- Foot Fractures
- Toe Fractures
- Sesamoid Fractures
- Metatarsal Fractures
- Compartment Syndrome
A fracture is a crack or break in a bone. Most fractures result from force applied to a bone.
Topic Resources


")





")
")

Fractures usually result from injuries or overuse.
The injured body part hurts (especially when it is used), is usually swollen, and may be bruised or look distorted, bent, or out of place.
Other injuries, such as blood vessel and nerve damage, compartment syndrome, infections, and long-lasting joint problems, may also be present or develop.
Doctors can sometimes diagnose fractures based on symptoms, the circumstances causing the injury, and results of a physical examination, but x-rays are usually needed.
Most fractures heal well and result in few problems, but how long they take to heal varies, depending on many factors, such as the person's age, the type and severity of the injury, and other disorders present.
Treatment depends on the type and severity of the fracture and may include pain relieving medication, PRICE (protection, rest, ice, compression, and elevation), maneuvers or procedures to move the fractured bone fragments back into their normal position (reduction), immobilization of the injured part (for example, with a cast or splint), and sometimes surgery.
Bones are part of the musculoskeletal system, which also includes muscles and the tissues that connect them (ligaments, tendons, and other connective tissue, called soft tissues). These structures give the body its form, make it stable, and enable it to move.


In addition to fractures, tissues of the musculoskeletal system can be damaged in the following ways:
The bones in joints may become completely separated from each other (called dislocation) or only partly out of position (called subluxation).
Ligaments (which attach bone to bone) can be torn (sprained).
Muscles can be torn (strained).
Tendons (which attach muscle to bone) can be torn (ruptured).
Sprains, strains, and ruptured tendons are called soft-tissue injuries.

Fractures (and other musculoskeletal injuries) vary greatly in severity and in the treatment needed. For example, fractures can range from a small, easily missed crack in a foot bone to a massive, life-threatening break in the pelvis.
Fractures can break the skin (called open fractures) or not (called closed fractures).


An injury that breaks a bone may also seriously damage other tissues, including the skin, nerves, blood vessels, muscles, and organs. These injuries can complicate treatment of the fracture and/or cause temporary or permanent problems.
Most often, the limbs are fractured, but fractures can occur in bones in any body part, such as the following:
How bones heal
When most tissues, such as those of the skin, muscles, and internal organs, are significantly injured, they mend themselves by producing scar tissue to replace the injured tissue. The scar tissue often looks different from normal tissue or interferes with function in some way. In contrast, bone heals by producing actual bone tissue.
When a bone heals itself after a fracture, the fracture often eventually becomes virtually undetectable. Even bones that have been shattered, when treated appropriately, can often be repaired and function normally.
How quickly bone heals depends on the person's age and other disorders present. For example, children heal much more quickly than adults. Disorders that interfere with blood flow (such as diabetes and peripheral arterial disease) slow healing.
Fractures heal in three overlapping stages:
Inflammation
Repair
Remodeling
In the inflammatory stage, healing begins immediately after the fracture. Cells of the immune system move to the injured area to remove damaged tissue, bone fragments, and blood that leaked from broken blood vessels.
The immune cells release substances that attract more immune cells, increase blood flow to the area, and cause more fluids to enter the damaged area. As a result, the area around the fracture becomes inflamed—red, swollen, and tender.
The inflammatory process peaks in a couple of days, but it takes weeks to subside. This process causes most of the pain people feel soon after a fracture.
During this stage and the repair stage, the fractured body part often needs to be kept from moving (immobilized)—for example, with a cast or splint.
The repair stage begins within days after the injury and lasts for weeks to months. New bone (called callus) is made to repair the fracture. At first, this new bone, called the external callus, does not contain any calcium (a mineral that gives bone its strength and density). This new bone is soft and rubbery. Thus, it can be damaged easily and may allow the healing bone to slip out of place (be displaced). Also, it cannot be seen on x-rays.
In the remodeling stage, bone is broken down, rebuilt, and restored to its former state. Remodeling takes many months. Calcium is deposited in the callus, which then becomes much stiffer and stronger and easier to see on x-rays, and the normal shape and structure of the bone are restored.
During this stage, people can gradually start to use the injured part normally. They should gradually resume their normal activities and gradually increase the amount of stress or weight they put on the injured part.
Causes of Fractures
Trauma is the most common cause of fractures. Trauma includes:
Direct force, as occurs in falls or motor vehicle crashes
Repeated moderate force, as may occur in long-distance runners or in soldiers marching with a heavy load on their back (such fractures are called stress fractures)
How severe a fracture is depends partly on how strong the force is. For example, a fall on level ground usually causes minor fractures, but a fall from a tall building can cause severe fractures that involve several bones.
Some fractures occur while playing certain sports (see Sports Injuries).
Some disorders can weaken bone. They include:
Certain infections
Bone tumors (which may be cancerous or not), including cancers that have spread (metastasized) from elsewhere in the body to the bone
People with one of these disorders are more likely to break a bone, even when only slight force is involved. Such fractures are called pathologic fractures.
Symptoms of Fractures
The most obvious symptom of a fracture is:
Pain
The injured part hurts, especially when people try to put weight on it or use it. The area around the fracture is tender to the touch. Other symptoms include:
Swelling
A part that looks distorted, bent, or out of place
Bruising or discoloration
Inability to use the injured part normally
Possibly loss of feeling (numbness or abnormal sensations)
Fractures typically cause swelling, but swelling may take hours to develop and, in some types of fractures, is very slight.
When muscles around the injured area try to hold a broken bone in place, muscle spasms may occur, causing additional pain.
Bruises appear when bleeding occurs under the skin. The blood may come from blood vessels in a broken bone or in the surrounding tissues. At first, the bruise is purplish black, then slowly turns green and yellow as the blood is broken down and reabsorbed back into the body. The blood can move quite a distance from the fracture, causing a large bruise or a bruise some distance from the injury. It can take a few weeks for blood to be reabsorbed. The blood can cause temporary pain and stiffness in the surrounding structures. For example, shoulder fractures can bruise the entire arm and cause pain in the elbow and wrist.
Pain, as well as the fracture itself, often prevents a person from moving the fractured part normally.
Because moving the injured part is so painful, some people are unwilling or unable to move it. If people (such as young children or older adults) cannot speak, refusal to move a body part may be the only sign of a fracture. However, some fractures do not keep people from moving the injured part. Being able to move an injured part does not mean that there is no fracture.
Complications of Fractures
Fractures can be accompanied by or lead to other problems (complications). However, serious complications are unusual. The risk of serious complications is increased if the skin is torn or if blood vessels or nerves are damaged.
Some complications (such as blood vessel and nerve damage, compartment syndrome, fat embolism, and infections) occur during the first hours or days after the injury. Others (such as problems with joints and healing) develop over time.
Blood vessel damage
Many fractures cause noticeable bleeding around the injury. Rarely, bleeding within the body (internal bleeding) or from an open wound (external bleeding) is massive enough to cause a life-threatening drop in blood pressure (shock). For example, shock may result when fractures of the thighbone (femur) or pelvis cause severe internal bleeding. If a person is taking a medication to prevent blood clots from forming (an anticoagulant), relatively minor injuries can cause substantial bleeding.
A dislocated hip or knee can disrupt blood flow to the leg. Thus, the tissues in the leg may not get enough blood (called ischemia) and may die (called necrosis). If enough tissue dies, part of the leg may have to be amputated. Sometimes fractures of the elbow or upper arm can disrupt blood flow to the forearm, causing similar problems. A disrupted blood supply may not cause any symptoms until several hours after the injury.
Nerve damage
Sometimes nerves are stretched, bruised, or crushed when a bone is fractured. A direct blow can bruise or crush a nerve. These injuries usually heal on their own over weeks to months to years, depending on the severity of the injury. Some nerve injuries never heal completely.
Rarely, nerves are torn, sometimes by sharp bone fragments. Nerves are more likely to be torn when the skin is torn. Torn nerves do not heal on their own and may have to be repaired surgically.
Pulmonary embolism
Pulmonary embolism is the most common severe complication of serious fractures of the hip or pelvis. It occurs when a blood clot forms in a vein in the leg or pelvis, breaks off (becoming an embolus), travels to a lung, and blocks an artery there. As a result, the body may not get enough oxygen.
Having a hip fracture greatly increases the risk of pulmonary embolism because it involves:
Injury to the leg, where most of the clots that cause pulmonary embolism form
Forced immobility (having to stay in bed) for hours or days, slowing blood flow and thus giving clots the opportunity to form
Swelling around the fracture, which also slows blood flow in the veins
About one third of people who die after a hip fracture die of pulmonary embolism. Pulmonary embolism is much less common when the lower leg is broken and is very rare when the arm is broken.
Fat embolism
Fat embolism rarely occurs. It can occur when long bones (such as the thighbone) are fractured and release fat from the bone's interior (marrow). The fat may travel through the veins, lodge in the lungs, and block a blood vessel there, causing fat embolism syndrome. As a result, the body does not get enough oxygen, and people may become short of breath and have chest pain. Their breathing may become rapid and shallow, and their skin may become mottled or blue. They may also have neurologic symptoms (such as feeling confused) and develop a rash.
Compartment syndrome
Rarely, compartment syndrome develops. For example, it may develop when injured muscles swell a lot after an arm or a leg is broken. Because the swelling puts pressure on nearby blood vessels, blood flow to the injured limb is reduced or blocked. As a result, tissues in the limb may be damaged or die, and the limb may have to be amputated. Without prompt treatment, the syndrome can be fatal. Compartment syndrome is more likely to occur in people who have certain fractures of the lower leg, certain arm fractures, or a Lisfranc fracture (a type of foot fracture).
Infections
If the skin is torn when a bone is broken, the wound may become infected, and the infection may spread to the bone (called osteomyelitis, which is very difficult to cure).
Joint problems
Fractures that extend into a joint usually damage the cartilage at the ends of bones in the joint (called joint surfaces). Normally, this smooth, tough, protective tissue enables joints to move smoothly. Damaged cartilage tends to scar, causing osteoarthritis, which makes joints stiff and limits their range of motion. The knee, elbow, and shoulder are particularly likely to become stiff after an injury, especially in older adults.
Physical therapy is usually needed to prevent stiffness and help the joint move as normally as possible. Surgery is often needed to repair the damaged cartilage. After such surgery, the cartilage is less likely to scar, and if scarring occurs, it tends to be less severe.
Some fractures can make a joint unstable, increasing the risk of repeated injuries and osteoarthritis. Appropriate treatment, often including a cast or splint, can help prevent permanent problems.
Uneven limbs
In children, if a growth plate in a leg is fractured, the affected leg may not grow normally and may be shorter than the other leg. Growth plates, which are made of cartilage, enable bones to lengthen until children reach their full height. If a fracture does not involve the growth plate, it may stimulate bone growth from the fracture site itself. If it stimulates growth, the fractured leg may grow too much and be longer than the other leg.
In adults, surgery to repair the thighbone may result in one leg that is longer than the other.
Problems with healing
Sometimes broken bones do not grow back together as expected. They may:
Not grow back together (called nonunion)
Grow back together very slowly (called delayed union)
Grow back in the wrong position (called malunion)
These problems are more likely to occur when:
The broken bones are not kept next to each other and are not kept from moving (meaning they are not immobilized with a cast or a splint).
The blood supply is disrupted.
Certain disorders, such as diabetes and peripheral vascular disease, and certain medications, such as corticosteroids, can delay or interfere with healing.
Osteonecrosis
When blood flow to a bone is disrupted, part of the bone may die, resulting in osteonecrosis. Certain injuries (such as scaphoid wrist fractures and hip fractures in which the broken bones are out of place) are more likely to cause osteonecrosis.
Diagnosis of Fractures
A doctor's evaluation
X-rays to identify fractures
Sometimes magnetic resonance imaging or computed tomography
If people think that they may have a broken bone, they should go or be taken to an emergency department. Possible exceptions are some toe or fingertip injuries.


Image courtesy of Danielle Campagne, MD.
People should also be taken to an emergency department, often by ambulance, if any of the following apply:
The problem is obviously serious (for example, if it resulted from a car crash or if people cannot use the affected body part).
They have several injuries.
They have symptoms of a complication—for example, if they lose sensation in the affected body part, they cannot move the affected part normally, the skin feels cool or turns blue, or the affected part is weak.
They cannot put any weight on the affected body part.
An injured joint feels unstable.
If injuries result from a serious accident, the doctor's first priority is:
To check for severe injuries and complications, such as an open wound, nerve damage, significant blood loss, disrupted blood flow, and compartment syndrome
For example, doctors do the following:
Measure blood pressure: Blood pressure is low in people who have lost a lot of blood.
Check pulses and the color and temperature of the skin: Absent or weak pulses and pale, cool skin may indicate that blood flow is disrupted. These symptoms may mean that an artery is damaged or that compartment syndrome has developed.
Check sensation in the skin to determine whether the person can feel normally: Doctors ask whether the person has abnormal sensations, such as a pins-and-needles sensation, tingling, or numbness. Abnormal sensations suggest nerve damage.
If any of these injuries and complications are present, doctors treat them as needed, then continue with the evaluation.
Description of the injury
Doctors ask the person (or a witness) to describe what happened. Often, the person does not remember how an injury occurred or cannot describe it accurately. Knowing how the injury occurred can help doctors determine the type of injury. For example, if a person reports that a snap or pop occurred, the cause may be a fracture (or an injury to a ligament or tendon). Also, doctors ask in which direction the joint was stressed during the injury. This information can help doctors determine which bones and other structures are damaged.
Doctors also ask when the pain started and how severe it is.
If it started immediately after the injury, the cause may be a fracture or a severe sprain.
If the pain began hours to days later, the injury is usually minor.
If the pain is more severe than expected for the injury or if the pain steadily worsens during the first hours after the injury, compartment syndrome may have developed or blood flow may be disrupted.
Physical examination
The physical examination includes the following (in order of priority):
Checking for damage to blood vessels near the injured body part—for example, by checking pulse and skin temperature and color
Checking for damage to nerves (for example, checking sensation) near the injured part
Examining and moving the injured part
Examining the joints above and below the injured part
Doctors gently feel the injured part to determine whether bones are in pieces or out of place and whether the area is tender. Doctors also check for swelling and bruising. If no swelling develops within several hours after the injury, a fracture is unlikely.
Doctors also ask whether the person can use, put weight on, and move the injured part.
Doctors test the stability of a joint by gently moving it, but if a fracture is possible, x-rays are done first to determine whether moving the joint is safe. Doctors check for grating or crackling sounds (crepitus) when the injured part is moved. These sounds may indicate a fracture.
Doctors also check the joint above and below the injured joint and check for ligament, tendon, and muscle injuries.
If pain or muscle spasms interfere with the examination, the person may be given a pain reliever and/or muscle relaxant by mouth or injection, or a local anesthetic may be injected into the injured area. Or the injured part may be immobilized until the spasms stop, usually for a few days, and then examined.
Tests
Imaging tests used to diagnosis fractures include:
X-rays
Magnetic resonance imaging (MRI)
Computed tomography (CT)
X-rays are the most important and usually the first and only test done to diagnose a fracture.
However, x-rays are not always needed, depending on which body part is affected and what doctors suspect. For example, if an injured body part (such as the toes, except the big toe) would be treated the same way regardless of whether it is fractured, x-rays are usually not needed.
X-rays are usually taken from at least two angles to show how the fragments of bone are aligned. These routine x-rays may not show small fractures when the pieces of broken bone remain in place (that is, they do not separate into fragments). Such fractures are called occult (hidden) fractures. So sometimes additional x-rays are taken from different angles. Occasionally, doctors wait to take x-rays for a few days or even weeks because some occult fractures, such as rib fractures, stress fractures, and scaphoid wrist fractures, become visible on x-rays only after the fracture begins to heal and calcium is deposited in the new bone.
When x-rays do not show a fracture, but doctors still suspect one, doctors may apply a splint and re-examine the person days later. If symptoms are still bothersome, they may take another x-ray. Fractures may be easier to see on x-rays after they have been healing for a while.
If x-rays show a fracture in a bone that looks abnormal (for example, if areas of bone look unusually thin), the fracture probably occurred because a disease (such as osteoporosis) weakened the bone.
CT or MRI may be done when:
Results of the examination strongly suggest a fracture but x-rays do not show one.
A specialist needs more detailed views of the fracture to determine the best way to treat it.
CT and MRI may also be done to provide more detail about fractures than routine x-rays can show. CT can show the fine details of a fractured joint surface and areas of a fracture that are covered by undamaged bone. CT and particularly MRI can show soft tissues, which are not usually visible on x-rays. MRI shows the tissues around the bone and thus helps detect injury to nearby tendons, ligaments, cartilage, and muscle. It can show changes caused by cancer. MRI also shows injury (swelling or bruising) within the bone and can thus detect small fractures before they appear on x-rays.
Other tests may be done to check for related injuries:
Angiography (x-rays or CT scans taken after a contrast agent, which can be seen on x-rays, is injected into arteries) to check for damaged blood vessels
Nerve conduction studies to check for damaged nerves
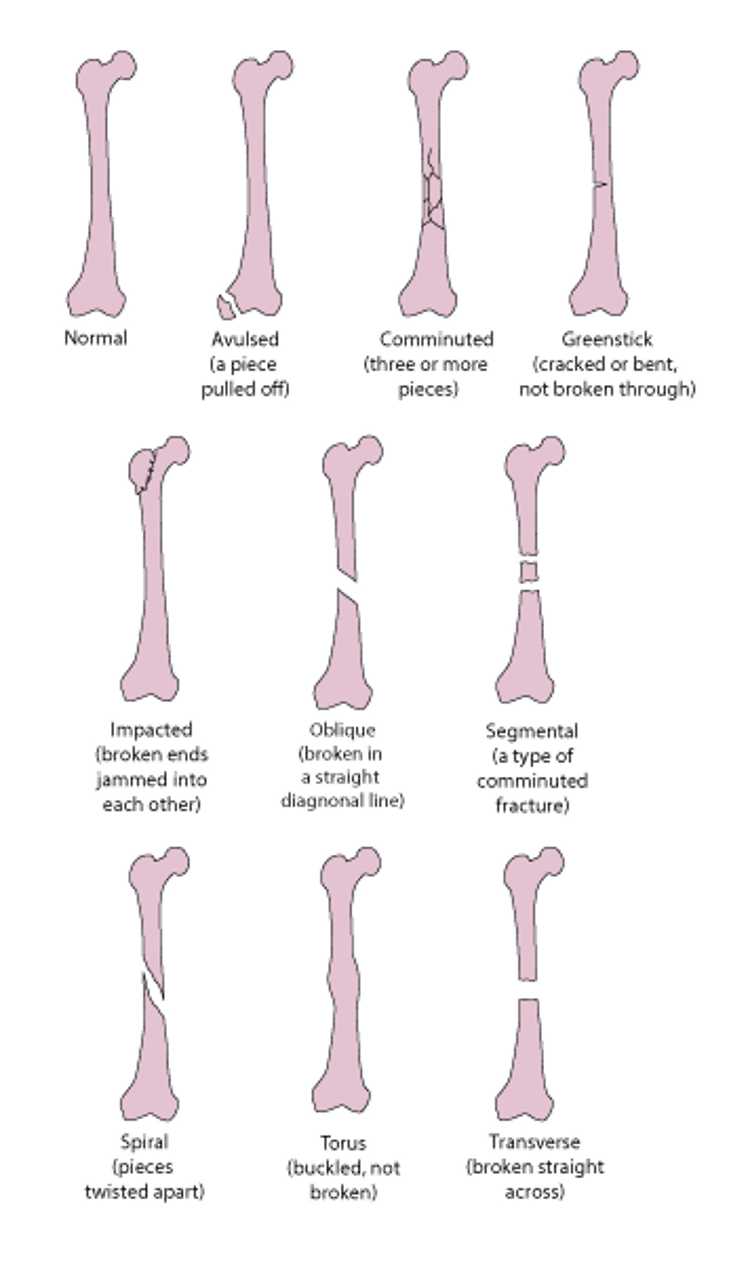
Types of fractures
Imaging tests enable doctors to identify the type of fracture and describe it precisely.
Deciphering Medical Terms for Fractures
Type | Description |
|---|---|
Angulated | The broken pieces of bone are not in a straight line. One is at an angle in relation to the other. |
Avulsion | A piece of bone is pulled off from the main part of the bone. A ligament may pull off a piece of bone if the external force is strong enough, as may occur in a fall. A tendon may pull off a piece of bone if the attached muscle contracts forcefully enough, as may occur in young athletes. Avulsion fractures usually occur in the hand, foot, ankle, knee, or shoulder. |
Closed | The skin over the fractured bone is not torn. |
Comminuted | The bone is broken into three or more pieces. Often, the bone is broken into many very small pieces. These fractures are often caused by a great force, as occurs in a car crash. They can also occur in people with osteoporosis, which weakens bone. |
The bone collapses into itself. These fractures usually occur in older adults (particularly those with osteoporosis). The backbones (vertebrae) are often affected (called vertebral crush fractures). | |
Displaced | Some parts or pieces of the broken bone are separated and not in correct alignment. |
Greenstick | The bone is partly cracked and/or bent but not completely broken through. Greenstick fractures occur only in children. |
These fractures occur in the growth plate, which is made of cartilage. Growth plates enable bones to lengthen until children reach their full height. When growth is completed, growth plates are replaced by bone. When a growth plate is fractured, the bone may stop growing or grow crookedly. Growth plate fractures occur only in children and adolescents. | |
Impacted | One end of the broken bone is jammed into the other. As a result, the bone appears shortened. |
Joint (intra-articular) | Fractures may extend into the cartilage at the ends of bones that form a joint (called joint surfaces). Normally, this cartilage reduces the amount of friction that occurs when bones in a joint rub against each other. When this cartilage is fractured, people cannot move the joint as well, and osteoarthritis is more likely to develop in the joint. |
Nondisplaced | The pieces of broken bone are still in place (aligned normally), and there is no space between them. |
Oblique | The bone is broken in a straight line diagonally across the long middle part (shaft) of the bone. |
Occult | These small fractures are difficult or impossible to see on x-rays, but they may be seen on other imaging tests such as computed tomography (CT) or magnetic resonance imaging (MRI). After a few days or weeks, changes occur in the new bone that forms as the bone heals. Then occult fractures may be seen on x-rays. Some stress fractures are occult. |
Open | The skin and tissues covering the fractured bone are torn, and the bone may be sticking out of the skin. Dirt, debris, or bacteria can easily contaminate the wound and may cause an infection in the broken bone. |
Osteoporotic | Osteoporotic fractures result from osteoporosis (progressive loss of bone density), which weakens bones and makes them more likely to break. Osteoporotic fractures (sometimes called fragility fractures) occur in older adults, usually in the hips, wrists, spine, shoulders, or pelvis. |
Pathologic | Pathologic fractures are caused by a disorder that weakens a bone, such as osteoporosis, certain bone infections, or bone tumors (including metastases to the bone from cancers elsewhere in the body to the bone). |
Segmental | There are two separate breaks in a bone. Segmental fractures are a type of comminuted fracture. |
Spiral (torsion) | Spiral fractures occur when the bone is twisted apart. As a result, the ends of the bone may be sharp, jagged, and slanted. |
A stress fracture occurs when force is repeatedly applied to a bone during certain activities, such as walking with a heavy pack or running. Stress fractures are often small cracks in bone (sometimes called hairline fractures). Stress fractures commonly occur in bones that bear weight, such as those of the foot or lower leg. | |
Torus | The bone buckles rather than breaks. Torus fractures usually occur only in children. Bones in children can buckle rather than break because their bones are more rubbery than those in adults. |
Transverse | The bone is broken straight across. |
Some Types of Fractures

Treatment of Fractures
Treatment of serious complications
Pain relief
Protection, rest, ice, compression, and elevation (PRICE)
Realignment (reduction) of parts that are out of place
Immobilization, usually with a splint or cast
Sometimes surgery
Serious fractures and serious related injuries and complications, if present, are treated immediately (for example, shock or compartment syndrome). Without prompt treatment, such injuries may get worse, becoming more painful and making loss of function more likely. These injuries can cause serious problems or even death.
If people think that they have a fracture or another severe injury, they should go or be taken to an emergency department. If they cannot walk or have several injuries, they should go by ambulance. Until they can get medical help, they should do the following:
Prevent the injured limb from moving (immobilize it) and support it with a makeshift splint, sling, or a pillow
Elevate the limb, above the level of the heart if possible, to limit swelling
Apply ice (wrapped in a towel or cloth) to control pain and swelling
Treatment of children
Fractures in children are often treated differently from those in adults because the bones in children are smaller, more flexible, less brittle, and still growing. Children’s fractures heal much faster and more perfectly than adult fractures do. Several years after most fractures in children, the bone can look almost normal on x-ray.
For children, doctors often prefer treatment with casts over surgery because:
Children have less stiffness after wearing a cast than adults do.
They are more likely to be able to move normally after being in a cast.
Surgery near a joint can damage the part of the bone that enables children to grow (the growth plate).
Treatment of serious injuries
In the emergency department, doctors check for injuries that require immediate treatment.
If the skin is torn, the wound is cleaned, usually after a local anesthetic is used to numb the area, and covered with a sterile dressing. Also, the injured person is given a vaccine to prevent tetanus and antibiotics to prevent infection.
To make sure the injured part is not deprived of blood, doctors surgically repair damaged arteries unless the arteries are small and blood flow is not affected.
Severed nerves are also repaired surgically, but this surgery can be delayed until several days after the injury if necessary. If nerves are bruised or damaged, they may heal on their own.
Pain relief
Pain is treated as soon as possible, typically with opioid pain relievers and/or acetaminophen or an anesthetic injected into nerves in the area (called a nerve block). A nerve block prevents the nerves from sending pain signals to the brain.Pain is treated as soon as possible, typically with opioid pain relievers and/or acetaminophen or an anesthetic injected into nerves in the area (called a nerve block). A nerve block prevents the nerves from sending pain signals to the brain.
Aspirin and other Aspirin and othernonsteroidal anti-inflammatory drugs (NSAIDs) are sometimes not recommended due to the risk of bleeding. However, if no operation is planned, NSAIDs can be used.
PRICE
PRICE refers to the combination of:
Protection
Rest
Ice
Compression (pressure)
Elevation
If people who have a fracture also have soft-tissue injuries, they may benefit from PRICE. PRICE is used to treat injured muscles, ligaments, and tendons.
Protection helps prevent further injury that could worsen the original one. It may involve limiting the use of the injured part, avoiding putting weight on the injured body part, using crutches, and/or wearing a splint or cast.
Rest prevents further injury and may speed healing.
Ice and compression minimize swelling and pain. Ice is enclosed in a plastic bag, towel, or cloth and applied for 15 to 20 minutes at a time, as often as possible during the first 24 to 48 hours. Usually, compression is applied to the injury with an elastic bandage.
Elevating the injured limb helps drain fluid away from the injury and thus reduces swelling. The injured limb is elevated above heart level for the first 2 days.
After 48 hours, people can periodically apply heat (for example, with a heating pad) for 15 to 20 minutes at a time. Heat may relieve pain. However, whether heat or ice is best is unclear, and what works best may vary from one person to another.

Reduction
Often, broken bones must be moved back into their normal position (realigned, or reduced). For example, reduction is usually necessary if:
Pieces of a broken bone have become separated.
Pieces of a broken bone are out of alignment.
Certain fractures in children do not need to be realigned because the bone, which is still growing, can correct itself.
If possible, reduction is done without surgery (called closed reduction), by manipulating the bones or bone fragments back into place. After reduction is done, doctors usually take x-rays to determine whether the fractured bones are in their normal position.
Some injuries must be realigned surgically (called open reduction).
Because reduction is usually painful, people are usually given pain relievers, sedatives, and/or an anesthetic before the procedure. The types of medications that are used depend on how severe the injury is and how reduction is to be done:
Closed reduction of minor fractures (such as those of the fingers or toes): A local anesthetic, such as lidocaine, injected near the injured part, may be all that is needed.Closed reduction of minor fractures (such as those of the fingers or toes): A local anesthetic, such as lidocaine, injected near the injured part, may be all that is needed.
Closed reduction of major fractures (such as those of the arm, shoulder, or lower leg): People may be given a sedative and pain relievers by vein. The sedative makes them drowsy but not unconscious. They may also be given a local anesthetic by injection. For example, if people have a shoulder dislocation, lidocaine may be injected into the shoulder joint.Closed reduction of major fractures (such as those of the arm, shoulder, or lower leg): People may be given a sedative and pain relievers by vein. The sedative makes them drowsy but not unconscious. They may also be given a local anesthetic by injection. For example, if people have a shoulder dislocation, lidocaine may be injected into the shoulder joint.
Open reduction: People are given a general anesthetic by injection or through a face mask, making them unconscious. This procedure is usually done in an operating room.
Immobilization
After being realigned, the injury must be kept from moving (be immobilized).
Casts, splints, or slings are usually used after closed reduction of a fracture.
Hardware devices, such as pins, screws, rods, and plates, are often used during open reduction of a fracture. This procedure is called open reduction and internal fixation (ORIF).
Immobilization reduces pain and helps with healing by preventing further injury to surrounding tissues. If a leg or an arm bone is fractured, immobilization may help prevent fat embolism. Immobilization is helpful for most moderate or severe fractures. Joints on both sides of the fracture are immobilized.
If immobilization lasts too long (for example, for more than a few weeks in young adults), the joint may become stiff, sometimes permanently, and muscles may shorten (causing contractures) or shrink (waste away, or atrophy). Blood clots may develop. Such problems can develop quickly, and contractures can become permanent, usually in older adults. Consequently, doctors encourage movement as soon as the fracture heals. They also tend to use treatments that enable older adults to walk as soon as possible (such as surgical repair of a hip fracture), rather than ones that require them to be immobilized for a long time (such as bed rest or a cast).
Physical therapists can advise people about what they can do while their injured part is immobilized to maintain as much strength, range of motion, and function as possible. After immobilization has ended, physical therapists can help people with exercises to strengthen and stabilize the injured part. These exercises can help prevent future injuries and impairment.
Whether immobilization is required and which technique is used depend on the type of fracture.
Most fractures are immobilized with a cast, splint, or sling until they heal. Without immobilization, the broken ends are likely to move, healing is slower, and the bones may not grow back together. If the broken bones have been separated or are out of alignment, they usually must be realigned (reduced) before being immobilized.
Casts are usually used for injuries that must be kept immobilized for weeks.
Did You Know...
|


Image courtesy of Danielle Campagne, MD.
To apply a cast, doctors wrap the injured part in cloth, then apply a layer of soft cottony material to protect the skin from pressure and rubbing. Over this padding, doctors wrap dampened plaster-filled cotton bandages or fiberglass strips, which harden when they dry. Plaster is often used to immobilize broken bones that have been separated because it molds well and is less likely to rub against the body. Fiberglass casts are stronger, lighter, and longer-lasting. After a week or so, the swelling goes down. Then, the plaster cast can sometimes be replaced with a fiberglass cast to fit the limb more snugly.
People who require a cast are given special instructions for its care. If a cast is not correctly cared for, problems can develop. For example, if the cast becomes wet, the protective padding under the cast may become wet, and drying it completely may be impossible. As a result, the skin can soften and break down, and sores may form. Also, if a plaster cast gets wet, it can fall apart and thus no longer protect and immobilize the injured area.
People are instructed to keep the cast elevated as much as possible at or above heart level, especially for the first 24 to 48 hours. They should also regularly flex and extend their fingers or wiggle their toes. These strategies help blood drain from the injured limb and thus prevent swelling.
If the cast causes persistent or worsening pain, feels excessively tight, or causes new numbness or weakness, people must contact a doctor or go to the emergency department immediately. These symptoms may be due to a developing pressure sore or compartment syndrome. In such cases, doctors may have to remove the cast and apply another one.
Taking Care of a Cast
|
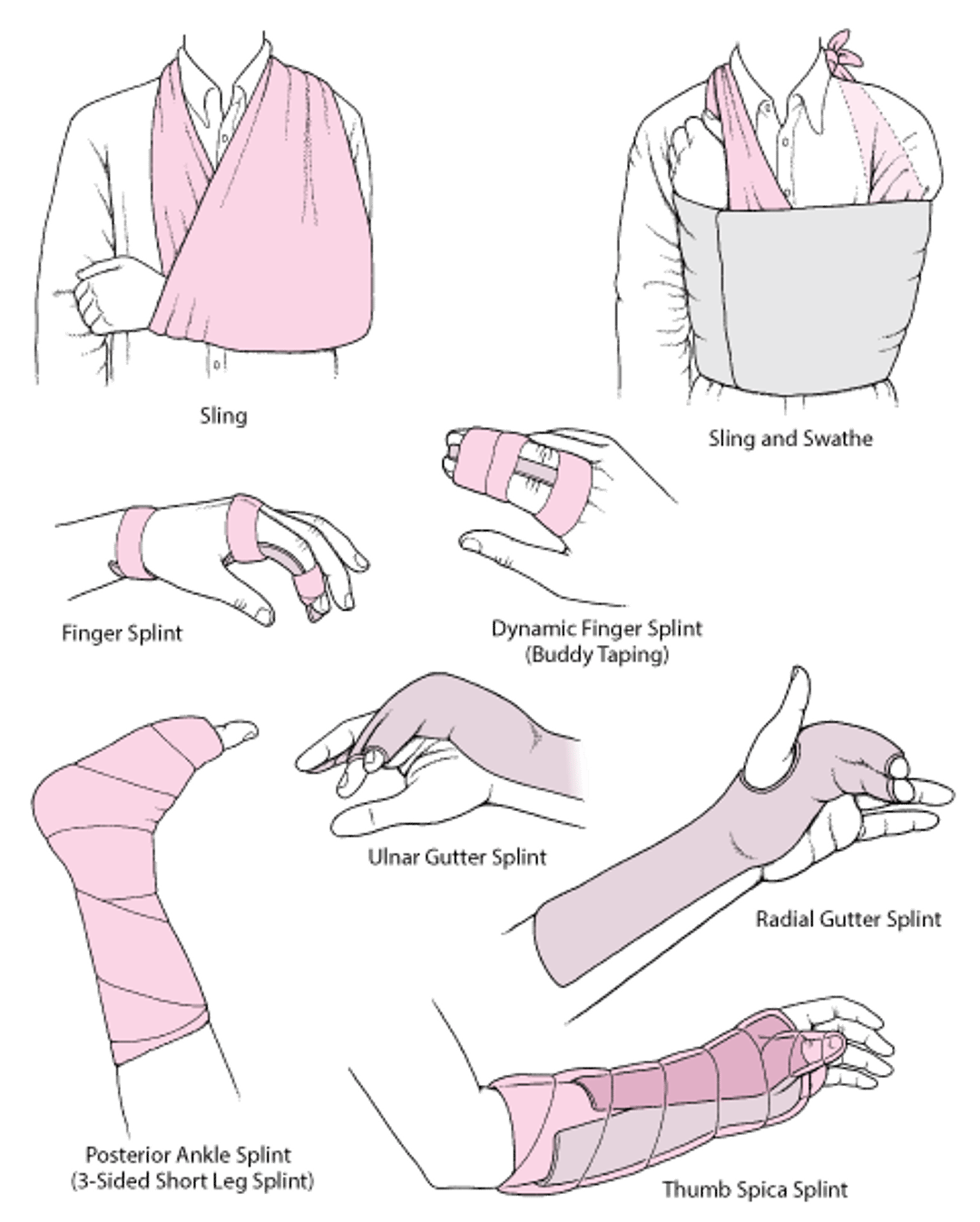
A splint can be used to immobilize some fractures, particularly if they need to be kept immobile for only a few days or less. Splints allow people to apply ice.
A splint is a long, narrow slab of plaster, fiberglass, or aluminum applied with elastic wrap or tape. Because the slab does not completely encircle the limb, there is room for some expansion in case the injured area swells. Thus, a splint does not increase the risk of developing compartment syndrome. Some injuries that eventually require a cast are first immobilized with a splint until most of the swelling resolves.
For finger fractures, aluminum splints lined with foam are commonly used.
A sling by itself can provide sufficient support and comfort for many shoulder and elbow fractures. The weight of the arm pulling downward helps keep many shoulder fractures aligned. Slings can be useful when complete immobilization has undesirable effects. For example, if a shoulder is completely immobilized, the tissues around the joint may become stiff, sometimes within days, preventing the shoulder from moving (called frozen shoulder). Slings limit movement of the shoulder and elbow but allow movement of the hand.
A swathe, which is a piece of cloth or a strap, may be used with a sling to prevent the arm from swinging outward, especially at night. The swathe is wrapped around the back and over the injured part.
Bed rest, which is occasionally required for fractures (such as some fractures of the spine or pelvis), can cause problems, including blood clots and a decrease in general physical fitness (deconditioning). Thus, bed rest is not commonly recommended.
Commonly Used Techniques for Immobilizing a Joint

Surgery
Sometimes fractures must be reduced and repaired surgically, as for the following:
Open fractures: Because the skin was broken, bacteria and debris can enter the body. Doctors must carefully clean the area around the fracture to remove all traces of debris. Doing so reduces the risk of infection.
Displaced fractures that cannot be aligned or kept aligned by closed reduction: When a piece of bone has shifted or a tendon is in the way, doctors may not be able to realign the broken bones by manipulating them from the outside (closed reduction). Or the fracture can be realigned using closed reduction, but the muscles pull on the pieces of bone and keep them from staying in place.
Joint surface fractures: These fractures extend into a joint, fracturing the cartilage at the ends of the bones in the joint. To prevent people from developing arthritis later, doctors must almost perfectly realign the fractured cartilage. Realignment can be more precise when it is done surgically.
Pathologic fractures in a bone weakened by cancer: Bone weakened by cancer may not heal normally after a fracture. Surgery may be needed to prevent the fragments of bone from becoming displaced. Also, stabilizing the joint surgically reduces the pain and enables people to use the joint more quickly.
Fractures known to require surgery: Certain kinds of fractures (such as hip fractures and thighbone fractures) are known to heal more rapidly and have a better outcome when they are surgically repaired.
Fractures that would otherwise require a long period of immobilization or bed rest: Surgery shortens the time people have to stay in bed. For example, surgery enables people who have had a hip fracture to get out of bed and begin walking soon after the operation, often as soon as the first day after surgery (with the help of a walker).
Complicated fractures: Surgery may be required to treat certain injuries that occur with a fracture, such as damaged arteries or severed nerves.
In open reduction with internal fixation (ORIF), surgery is done to restore the bone’s original shape and alignment. X-rays are used to help surgeons see how to align the bones. After making an incision to expose the fracture, the surgeon uses special instruments to align the bone fragments. Then, the fragments are held in place using some combination of metal wires, pins, screws, rods, and plates. For example, metal plates may be shaped as needed and attached to the outside of the bone with screws. Metal rods may be inserted from one end of the bone into the interior of the bone (marrow). These hardware devices are made of stainless steel, high-strength alloy metal, or titanium. The devices that have been made in the last 15 to 20 years do not interfere with the strong magnets used in magnetic resonance imaging (MRI). Most do not set off security devices at airports. Some of these devices are permanently left in place, and some are removed after the fracture has healed.
Joint replacement (arthroplasty) may be needed, usually when fractures severely damage the upper end of the thighbone (femur), which is part of the hip joint, or the upper arm bone (humerus), which is part of the shoulder joint.
In bone grafting, doctors use chips of bone taken from another part of the body (such as the pelvis). This procedure may be done immediately if the gap between pieces of bone is too large. It may be done later if the healing process has slowed (delayed union) or stopped (nonunion).
Rehabilitation and Prognosis for Fractures
Most injuries heal well and result in few problems. However, some do not completely heal even though they are diagnosed and treated appropriately.
How long a fracture takes to heal varies from weeks to months depending on:
Type of fracture
Location of the fracture
The person's age
The presence of disorders that may delay healing
For example, children heal much faster than adults, and certain disorders (including those that cause problems with circulation, such as diabetes and peripheral vascular disease), slow healing.
People usually feel some discomfort during activities even after a fracture has healed enough to allow them to put their full weight on the injured part. For example, after about 2 months, a fractured wrist may be strong enough to use. However, the bone is still being rebuilt (remodeled). Thus, forceful gripping with the wrist may be painful for up to a year. Some people also notice that the injured part is more painful and stiffer when the weather is cold.
Being immobilized makes joints stiff, and muscles weaken and shrink because they are not used. If a limb is immobilized in a cast, the affected joint becomes stiffer each week, and eventually people become unable to fully extend and flex their limb. Such problems can develop quickly and become permanent, usually in older adults. After wearing a long leg cast (upper thigh to the toes) for a few weeks, the muscles usually shrink so much that people can insert their hand into the formerly tight space between the cast and their thigh. When the cast is removed, their muscles are very weak and look noticeably smaller.
To prevent or minimize stiffness and to help people maintain muscle strength, doctors may recommend surgery (open reduction and internal fixation [ORIF]) because after surgery, people are able to move the injured part relatively soon. Doctors may also recommend daily exercise, including range-of-motion exercises and muscle-strengthening exercises. While the fracture is healing, people can exercise the rest of their body.
After the fracture has healed sufficiently, the cast can be removed, and people can start exercising the injured limb. When exercising, they should pay attention to how the injured limb feels and avoid exercising too forcefully. If the muscles are too weak for people to exercise them or if such exercise could re-separate a fractured bone, a therapist moves their limbs for them (called passive exercise—see figure Increasing the Shoulder's Range of Motion). However, ultimately, to regain full strength of an injured limb, people must move their own muscles (called active exercise).
Spotlight on Aging: Injuries to Muscles, Bones, and Other Tissues
People who are over 65 are more likely to fracture bones for the following reasons:
In older adults, fractures often affect the ends of long bones, such as those in the forearm, upper arm, lower leg, and thigh. Fractures of the pelvis, spine (vertebrae), and wrist are also common among older adults. In older adults, recovery is often more complicated and slower than it is in younger people because
Even minor fractures can greatly interfere with older adult’s ability to do normal daily activities, such as eating, dressing, bathing, and even walking, especially if they used a walker before the injury. Immobilization: Being immobilized is a particular problem in older adults. In older adults, being immobilized is more likely to cause
Pressure sores develop when blood flow to an area is cut off or greatly reduced. In older adults, blood flow to a limb may already be reduced. When the weight of an injured limb rests on a cast, blood flow is reduced even more, and pressure sores may form. If bed rest is required, pressure sores can develop on areas of skin that touch the bed. These areas should be diligently inspected for any sign that the skin is breaking down. Because immobilization is more likely to cause problems in older adults, treatment of fractures focuses on helping older adults return to daily activities as quickly as possible rather than making sure that the fractured bone is perfectly aligned. To shorten the time people are immobilized and to help them return to daily activities sooner, doctors are increasingly using surgery to repair or replace a broken hip. People are instructed to move and walk (usually with help of a walker), often as soon as the first day after surgery. Physical therapy (for example, after a hip fracture) is also started. If hip fractures are not treated surgically, they require months of immobilization in bed before people are strong enough to bear weight. |







