




Coronary artery disease is a condition in which the blood supply to the heart muscle is partially or completely blocked.
The heart muscle needs a constant supply of oxygen-rich blood. The coronary arteries, which branch off the aorta just after it leaves the heart, deliver this blood. Coronary artery disease that narrows one or more of these arteries can block blood flow, causing chest pain (angina) or a heart attack (also called myocardial infarction, or MI).
In high-income countries, coronary artery disease is the leading cause of death in both men and women, accounting for about one third of all deaths. Coronary artery disease, specifically coronary atherosclerosis (literally “hardening of the arteries”), involves fatty deposits in the artery walls and may progress to narrowing and even blockage of blood flow in the artery). The death rate increases with age and overall is higher for men than for women, particularly between the ages of 35 and 55 years. After age 55, the death rate for men declines, and the rate for women continues to climb. After age 70 to 75 years, the death rate for women is similar to that for men who are the same age.
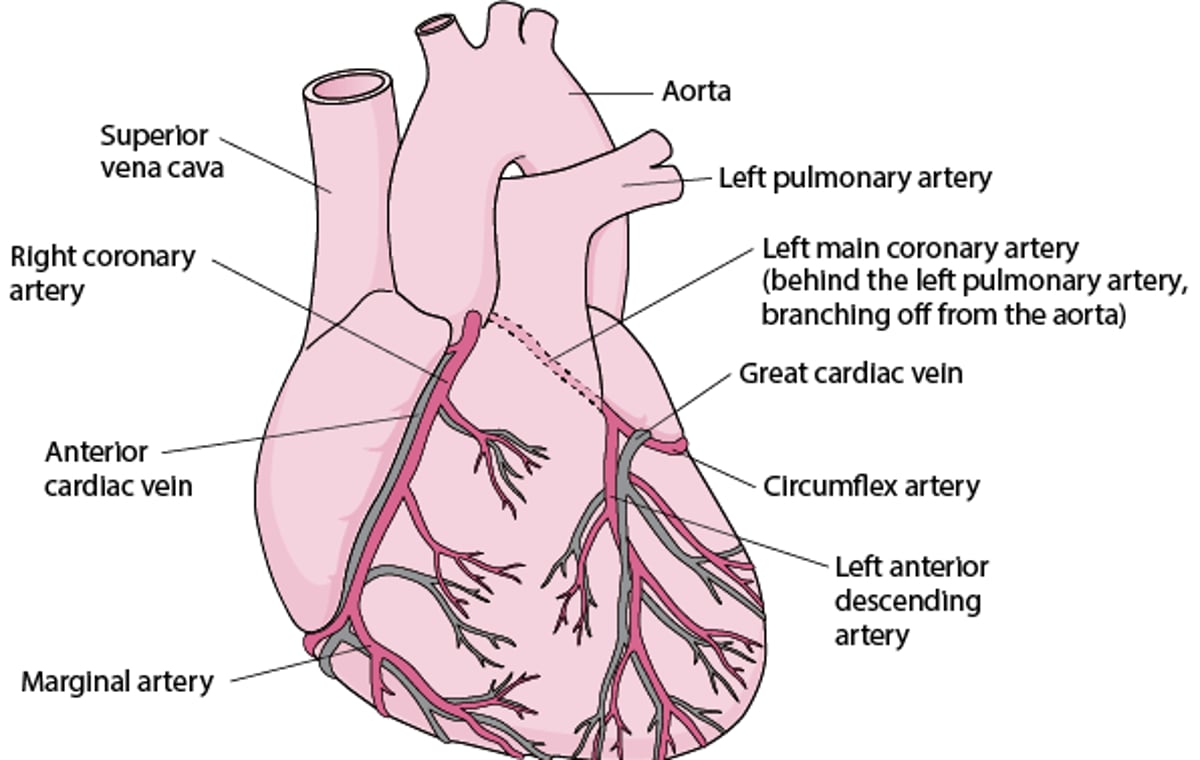
Supplying the Heart With Blood
Like any other tissue in the body, the muscle of the heart must receive oxygen-rich blood and have waste products removed by the blood. The right coronary artery and the left coronary artery, which branch off the aorta just after it leaves the heart, deliver oxygen-rich blood to the heart muscle. The right coronary artery branches into the marginal artery and the posterior interventricular artery, located on the back surface of the heart. The left coronary artery (typically called the left main coronary artery) branches into the circumflex and the left anterior descending artery. The cardiac veins collect blood containing waste products from the heart muscle and empty it into a large vein on the back surface of the heart called the coronary sinus, which returns the blood to the right atrium. |

Causes of Coronary Artery Disease
Coronary artery disease is almost always due to the gradual buildup of cholesterol and other fatty materials (called atheroma or atherosclerotic plaque) in the wall of a coronary artery. This process is called atherosclerosis and can affect many arteries, not just those of the heart.
The most common reason for abnormal reduction in blood flow to the heart is
Atherosclerosis
Other causes of abnormal blood flow reduction to the heart include
Spasm of a coronary artery, which can occur spontaneously or result from use of certain drugs such as cocaine and nicotine
Endothelial dysfunction, which means that a coronary blood vessel does not widen (dilate) in response to a need for increased blood flow (such as during exercise), resulting in less blood flow than the heart needs
Birth defects (for example, coronary artery abnormalities)
Coronary artery dissection (a tear running down the lining of a coronary artery)
Systemic lupus erythematosus (lupus)
Inflammation of the arteries (arteritis)
A blood clot that traveled from a heart chamber into one of the coronary arteries
Physical damage (due to an injury or radiation therapy)
As an atheroma grows, it may bulge into the artery, narrowing the interior (lumen) of the artery and partially blocking blood flow. With time, calcium accumulates in the atheroma. As an atheroma blocks more and more of a coronary artery, the supply of oxygen-rich blood to the heart muscle (myocardium) can become inadequate. The blood supply is more likely to be inadequate during exertion, when the heart muscle requires more blood. An inadequate blood supply to the heart muscle (due to any cause) is called myocardial ischemia. If the heart does not receive enough blood, it can no longer contract and pump blood normally.
An atheroma, even one that is not blocking very much blood flow, may rupture suddenly. The rupture of an atheroma often triggers the formation of a blood clot (thrombus). The clot further narrows or completely blocks the artery, causing acute myocardial ischemia. The consequences of this acute ischemia are referred to as acute coronary syndromes. These syndromes include unstable angina and 2 types of heart attack, depending on the location and degree of the blockage. In a heart attack, the area of the heart muscle supplied by the blocked artery dies (called myocardial infarction).
Risk Factors for Coronary Artery Disease
Some factors that affect whether a person develops coronary artery disease cannot be modified. They include
Advancing age
Male sex
Family history of early coronary artery disease (that is, having a close relative who developed the disease before age 55 years in the case of a male relative or 65 years in the case of a female relative)
Other risk factors for coronary artery disease can be modified or treated. These factors include
High blood levels of low-density lipoprotein (LDL) cholesterol (see Dyslipidemia)
High blood levels of lipoprotein a
Low blood levels of high-density lipoprotein (HDL) cholesterol
Smoking
Physical inactivity
Dietary factors
High blood levels of C-reactive protein (CRP)
Smoking more than doubles the risk of developing coronary artery disease and having a heart attack. Secondhand smoke appears also to increase risk.
Dietary risk factors include a diet that is low in fiber, vitamins C, D, and E, and phytochemicals (which are present in fruits and vegetables and are thought to promote health). For some people, a diet low in fish oils (omega-3 polyunsaturated fatty acids) increases risk.
Certain metabolic disorders, such as hypothyroidism, hyperhomocysteinemia (a very high level of the amino acid homocysteine in the blood), and a high level of apolipoprotein B (apo B), which is important in how the body manages fats, also are risk factors.
Whether infection with certain organisms contributes to the development of coronary artery disease is uncertain.
Treatment of Coronary Artery Disease
Doctors try to do 3 things for people with coronary artery disease. They try to
Reduce the heart’s workload
Improve blood flow through the coronary arteries
Slow down or reverse the buildup of atherosclerosis
The heart’s workload can be reduced by controlling the person’s blood pressure and using certain medications such as beta-blockers or calcium channel blockers that keep the heart from pumping too hard (see Medications for Treatment of Coronary Artery Disease).
Modifying the diet, exercising, and taking certain medications can help reverse atherosclerosis. These measures are the same as those used for the prevention of atherosclerosis.
Percutaneous Coronary Intervention
Percutaneous coronary intervention or PCI (also called percutaneous transluminal coronary angioplasty—PTCA) is used for people with an acute coronary syndrome (ACS) or for some people with angina that is not controlled sufficiently with medications.
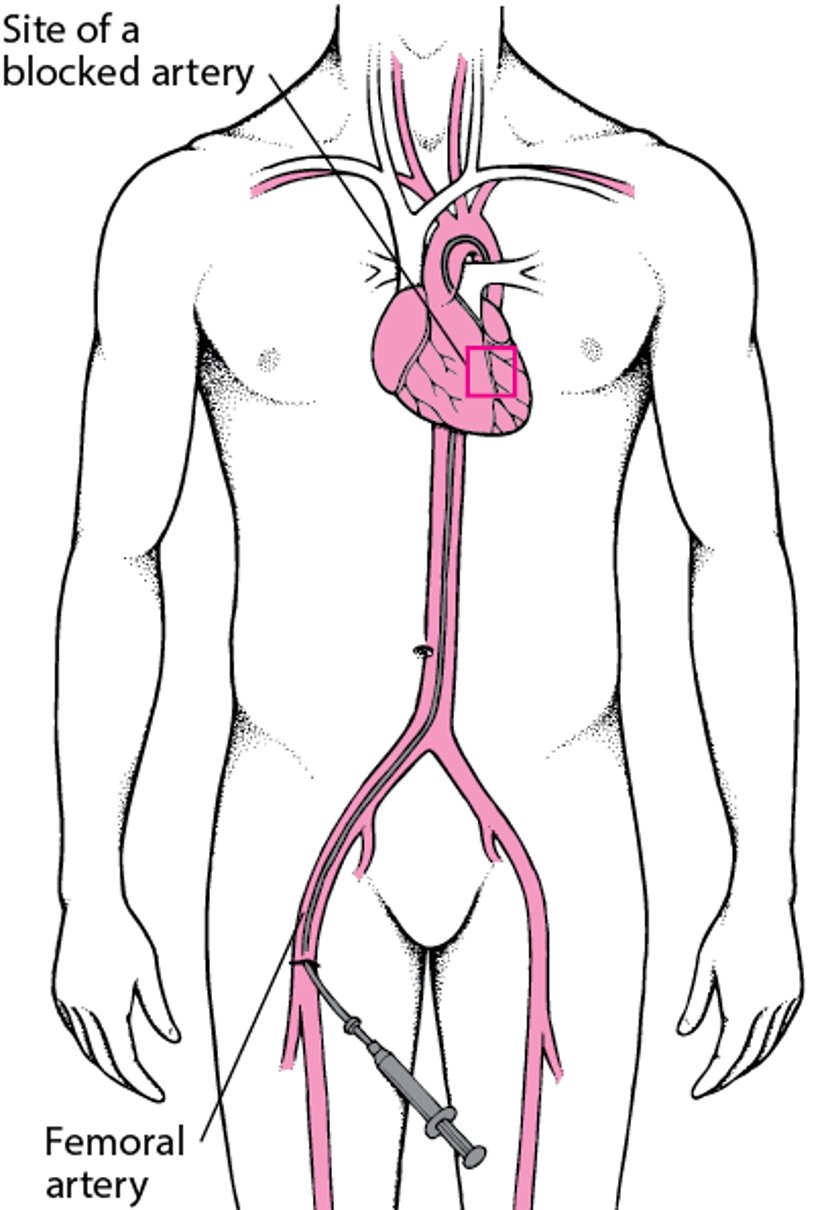
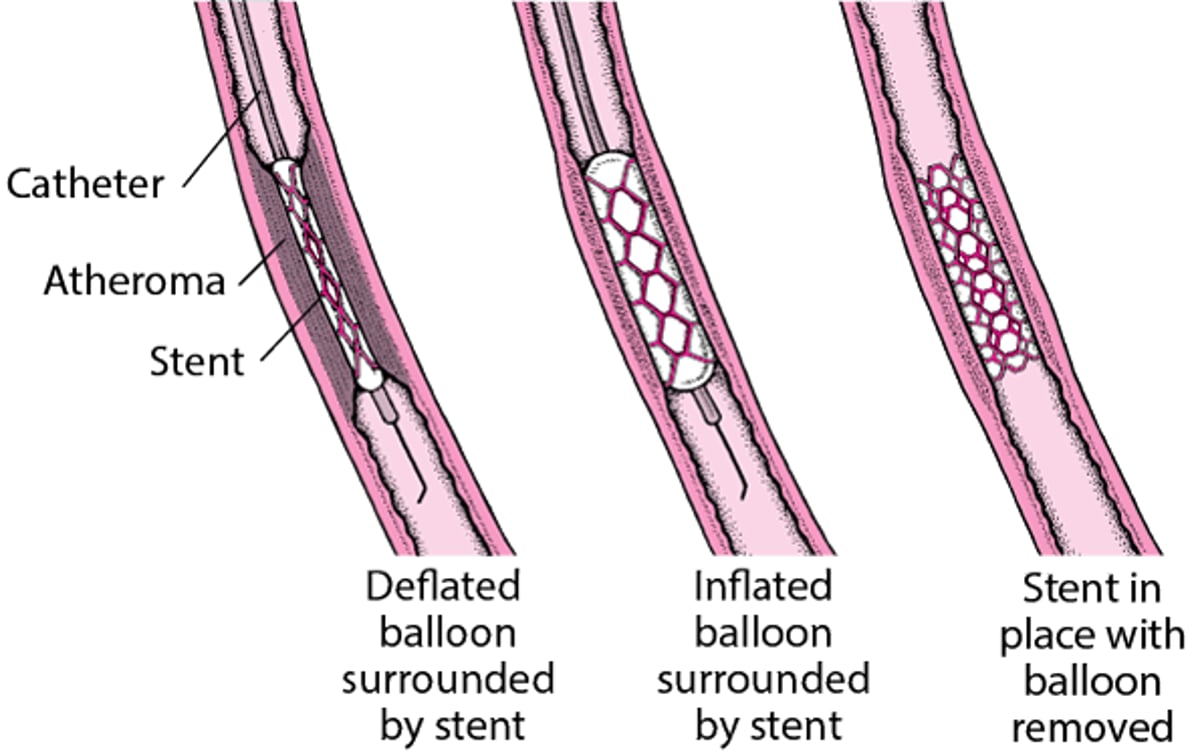
In PCI, doctors insert a needle into an artery in the wrist (radial artery) or into the main artery of the thigh (femoral artery). Then a long guide wire is threaded through the needle, into the artery, and up through the aorta into the narrowed coronary artery. A catheter with a balloon attached to the tip is threaded over the guide wire and into the narrowed coronary artery. The catheter is positioned so that the balloon is at the level of the narrowing. The balloon is then inflated for several seconds. The inflated balloon stretches the artery and compresses the atheroma that is narrowing the artery and so widens the artery. Inflation and deflation may be repeated several times.

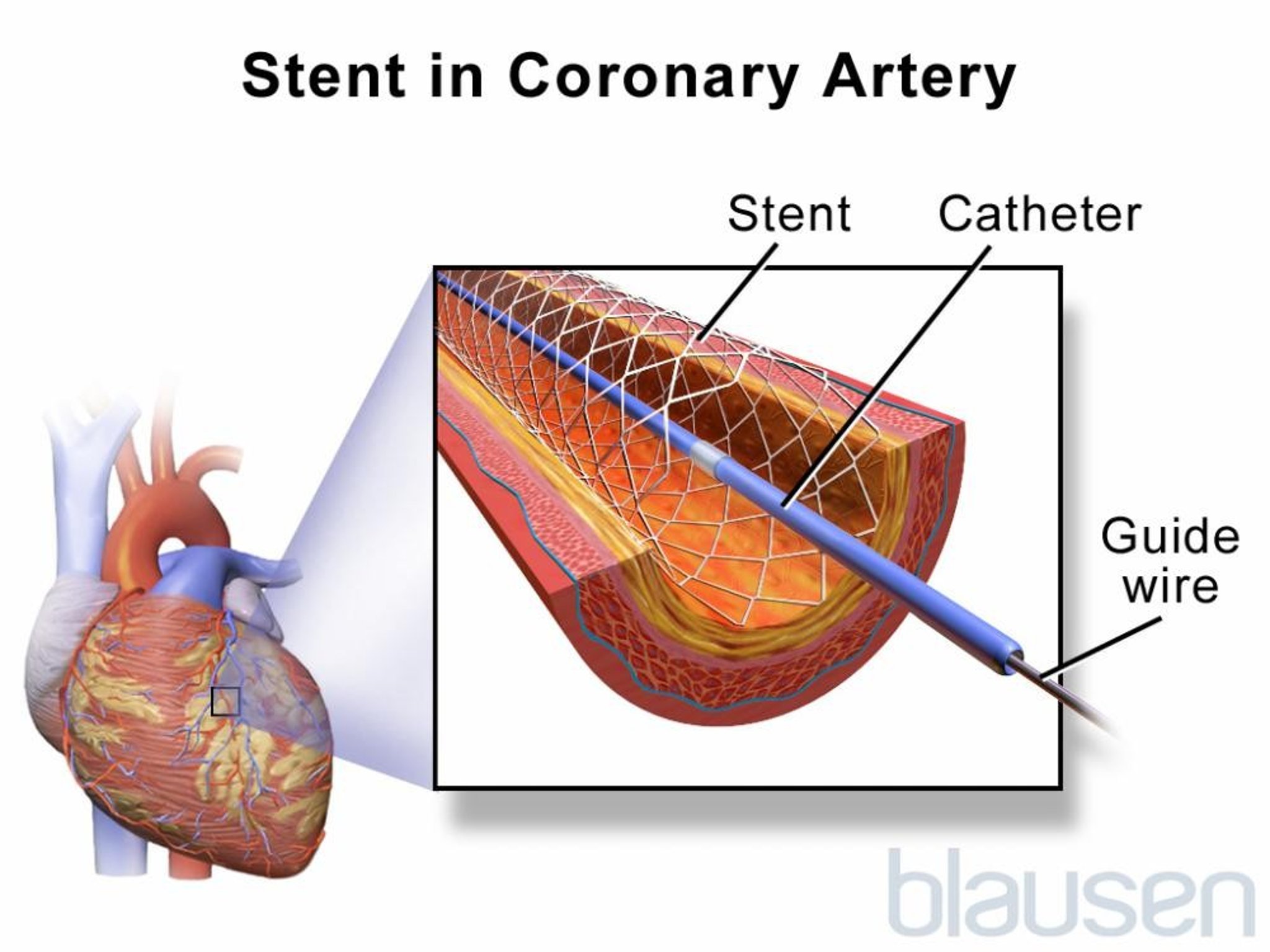
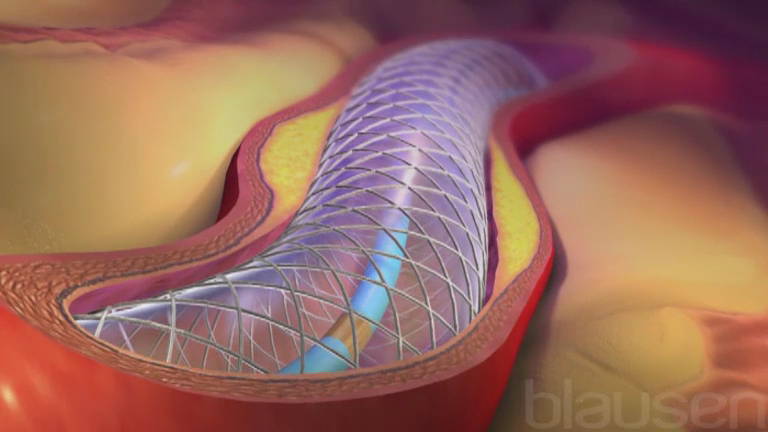
To help keep the coronary artery open, doctors typically insert a tube made of wire or manufactured mesh (a stent) into the artery. Most of the time, doctors use stents that are coated with a medication (called drug-eluting stents). The medication is released slowly to help prevent the coronary artery from becoming blocked again, a common problem with stents that are not coated (called bare-metal stents). However, although these drug-eluting stents are very helpful in keeping the artery open, people who have a drug-eluting stent have a slightly higher risk of developing a blood clot in the stent than do people who have a bare-metal stent. To decrease the risk of such clots, people who have a stent are given aspirin plus another antiplatelet agent (medications that stop platelets from clumping together to form clots) for at least 3 to 12 months after the stent is inserted. Often doctors start giving the antiplatelet agent before the stent is inserted. If the artery becomes blocked again, whether due to a clot or other causes, doctors may do a second PCI.
For many people, PCI is preferred to coronary artery bypass surgery (CABG) because it is a less invasive procedure with a shorter recovery time. However, the affected area of the coronary artery may not be suited to PCI because of its location, its length, the amount of calcium that accumulates, or other conditions. In addition, people with several areas of narrowing or other conditions may survive longer after CABG than after PCI. Thus, doctors carefully determine whether a person is a good candidate for the procedure.
Understanding Percutaneous Coronary Intervention (PCI)
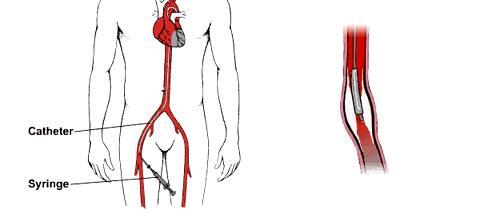
Doctors insert a balloon-tipped catheter into a large artery (sometimes the femoral artery, but the radial artery in the wrist is used most commonly) and thread the catheter through the connecting arteries and the aorta to the narrowed or blocked coronary artery. Then doctors inflate the balloon to force the atheroma against the arterial wall and thus open the artery. Usually, a collapsed tube made of wire mesh (a stent) is placed over the deflated balloon at the catheter’s tip and inserted with the catheter. When the catheter reaches the atheroma, the balloon is inflated, opening up the stent. Then the balloon-tipped catheter is removed, and the stent is left in place to help keep the artery open. | |
People are usually awake during the procedure, but doctors may give a medication to help them relax. People are closely monitored during PCI because balloon inflation momentarily blocks blood flow in the affected coronary artery. This blockage can cause chest pain and changes in the heart’s electrical activity (detected by ECG) in some people. | |


Coronary Artery Bypass Grafting
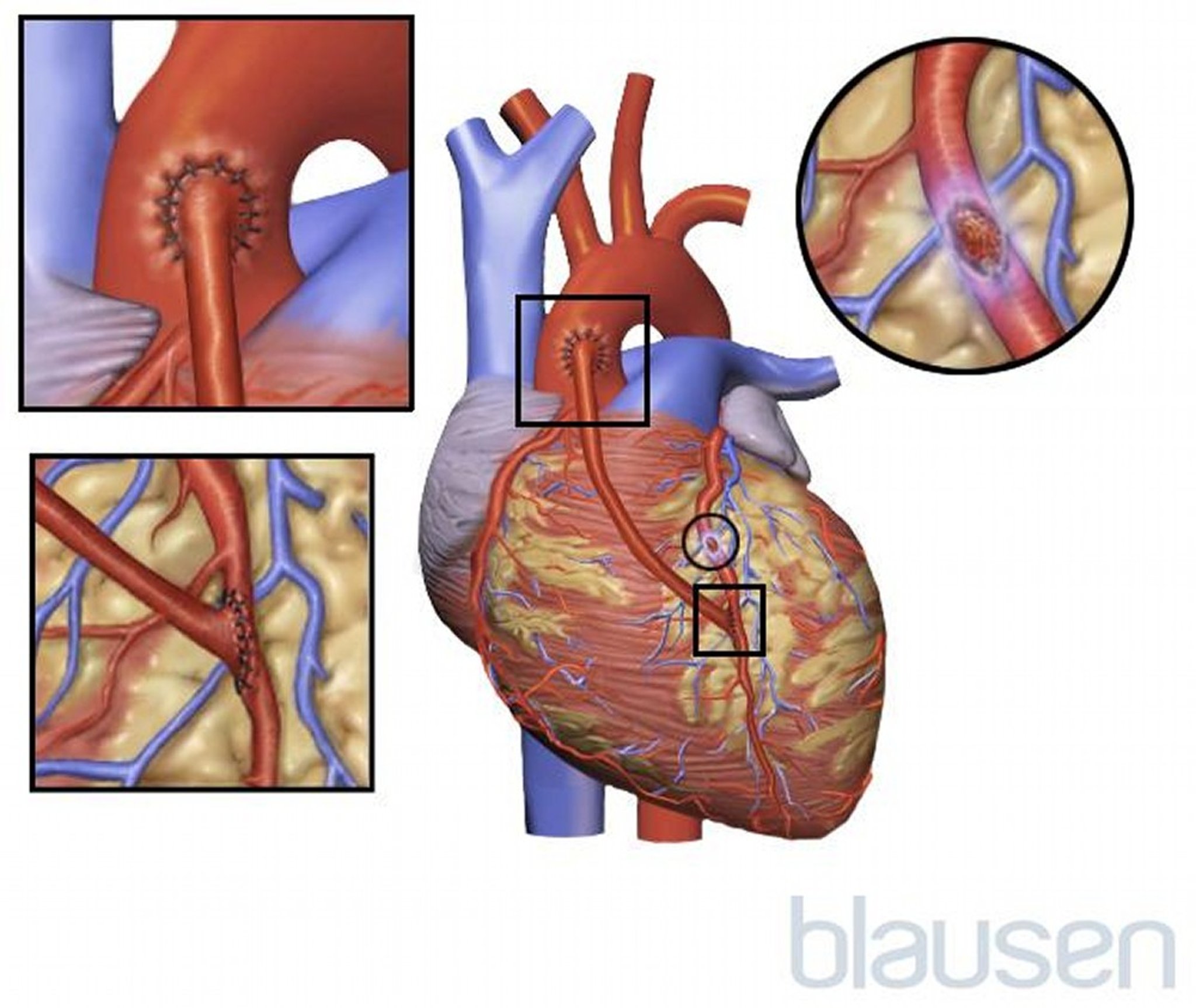
Coronary artery bypass grafting (CABG) is also called bypass surgery or coronary artery bypass surgery. In the procedure, doctors take an artery or vein from another part of the body to connect the aorta (the major artery that takes blood from the heart to the rest of the body) to a coronary artery past the point of its blockage. Blood flow is thus rerouted, skipping over (bypassing) the narrowed or blocked area. Veins are usually taken from the leg. Arteries are usually taken from beneath the breastbone (sternum) or from the forearm. Artery grafts rarely develop coronary artery disease, and more than 97% of them still work properly 10 years after the bypass surgery. However, vein grafts may gradually become narrowed by atheroma. After 1 year about 15% are completely blocked, and after 5 years, one third or more may be completely blocked.

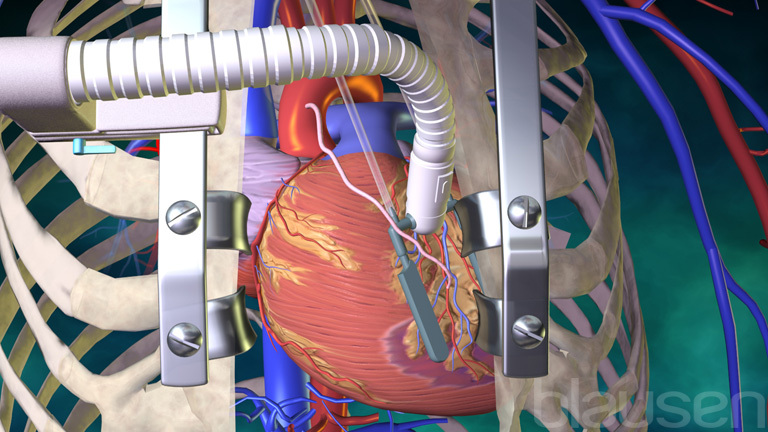
The surgery takes several hours, depending on the number of blood vessels to be grafted. A numeric modifier (for example, triple or quadruple) before bypass refers to the number of arteries (for example, 3 or 4) that are bypassed. The person is given a general anesthetic. Then, an incision is made down the center of the chest from the neck to the top of the stomach, and the breastbone is parted. This type of surgery is called open-heart surgery. Sometimes special equipment that permits the use of smaller incisions that do not split the breastbone is used.
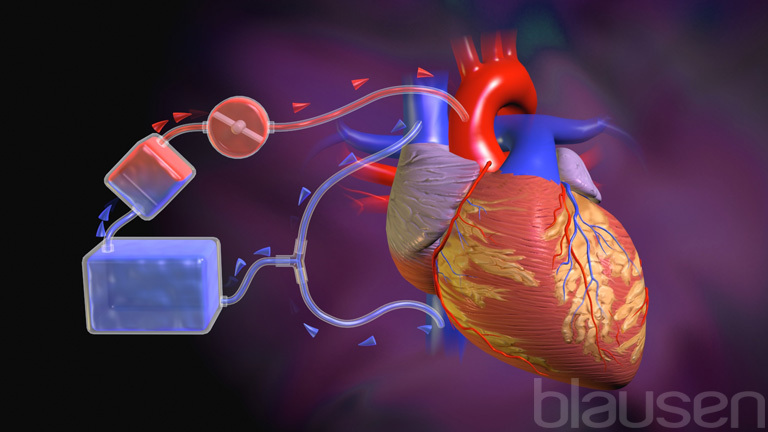
Usually, the heart is stopped so that it is not moving and thus is easier to operate on. A heart-lung machine is then used to put oxygen into the blood and pump the blood through the bloodstream. When only one or two blood vessels require grafting, the heart may be left pumping. This procedure is called an off-pump or beating-heart bypass procedure. The hospital stay is typically about 5 days, usually less if a heart-lung machine was not used during surgery. However, long-term results are the same with both procedures.
The risks due to surgery include stroke and heart attack. For people who have a normal-sized and normally functioning heart, have never had a heart attack, and have no additional risk factors, risk is less than 5% for a heart attack during surgery, 1 to 2% for stroke, and less than 1% for death. Risk is somewhat higher for people with reduced pumping ability of the heart (poor left ventricular function), damaged heart muscle from a previous heart attack, or other cardiovascular problems. However, if these people survive the surgery, their prospects for long-term survival are improved.
Some people develop changes in thinking or behavior after a CABG procedure. The changes may be mild or very severe and some may last for weeks to years. Older adults are at greater risk. Risk may decrease if a heart-lung machine is not used.
Other techniques
In minimally invasive bypass surgery (sometimes this type of surgery is called a keyhole procedure), chest incisions can be much smaller.
Some minimally invasive techniques involve robotics. While sitting at a computer console, a surgeon uses pencil-sized robotic arms to do the operation. The arms hold specially designed surgical instruments that can do intricate movements, mimicking those of the surgeon’s hands. Through a viewing scope, the surgeon watches a magnified 3-dimensional image of the operation. The operation requires three 1-inch (about 2 ½-centimeter) incisions—one for each of the two robotic arms and one for a camera, which is connected to the scope. Thus, the surgeon does not need to split open the person’s breastbone. The operating time and hospital stay are usually shorter than with open-heart surgery.
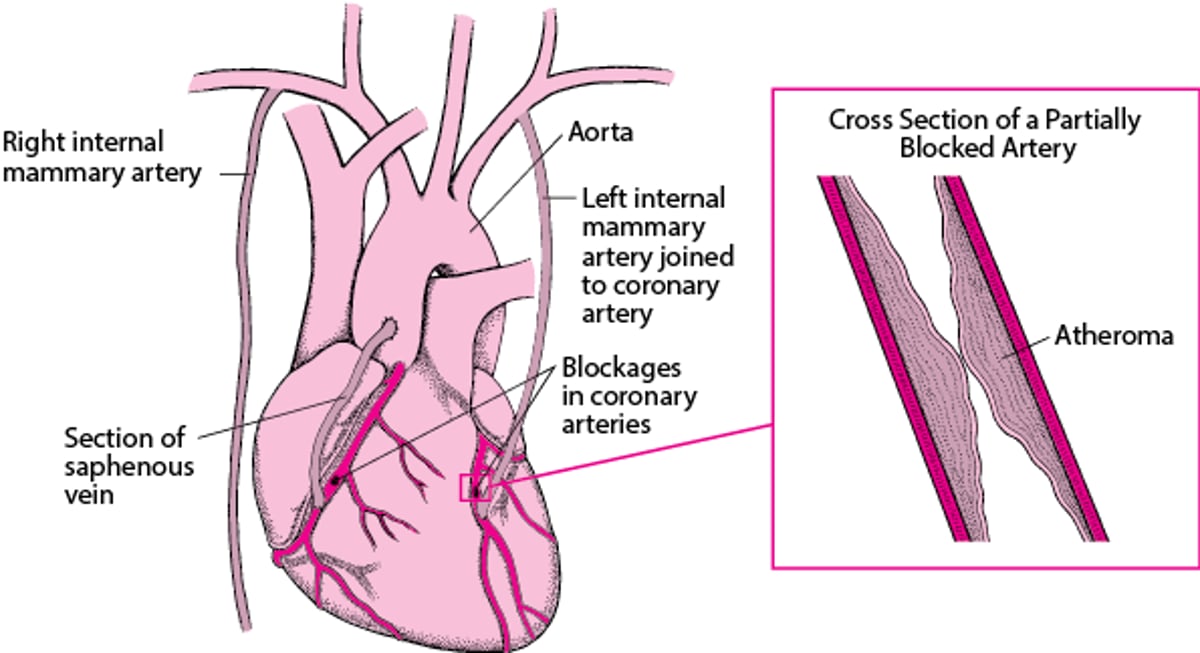
Coronary Artery Bypass Grafting
Coronary artery bypass grafting consists of attaching an artery or part of a vein to a coronary artery, so that the blood has an alternate route from the aorta to the heart muscle. As a result, the narrowed or blocked area is bypassed. An artery is preferred to a vein because arteries are less likely to become blocked later. In one type of bypass grafting, one of the two internal mammary arteries is cut, and one of the cut ends is attached to a coronary artery beyond the blocked area. The other end of this artery is tied off. If an artery cannot be used or if there is more than one blockage, a section of a vein—usually, from the saphenous vein, which runs from the groin to the ankle—is used. One end of the section (graft) is attached to the aorta, and the other to a coronary artery beyond the blocked area. Sometimes a vein graft is used in addition to the mammary artery graft. |

Prevention of Coronary Artery Disease
Modifying risk factors of atherosclerosis can help prevent coronary artery disease. Some of these factors are interrelated, so that modifying one also modifies another.
Smoking
Quitting smoking is most important. People who quit smoking decrease their risk of developing coronary artery disease by half compared with those who continue to smoke. How long people smoked before quitting does not matter. Quitting also decreases the risk of death after coronary artery bypass surgery or after a heart attack. Avoiding secondhand smoke is also important.
Diet
Several changes are beneficial:
Less saturated fat
No trans fats
More fruits and vegetables
More fiber
Moderate (if any) alcohol
Less simple carbohydrates (such as, sugar, white bread, and white flour)
Limiting the amount of fat to no more than 25 to 35% of daily calories is recommended to promote good health. However, some experts believe that fat must be limited to 10% of daily calories to reduce the risk of coronary artery disease. A low-fat diet also helps lower total and LDL (the bad) cholesterol levels, another risk factor for coronary artery disease. The type of fat consumed is as important as the amount of fat. Thus, eating oily fish, such as salmon, which are high in omega-3 fats (good fats), regularly and strictly avoiding the more harmful trans fats are recommended. In the United States and some other nations, trans fats have been banned in packaged food products, fast food sites, and restaurants.
Eating at least 5 servings of fruits and vegetables daily can decrease the risk of coronary artery disease. Such foods contain many phytochemicals. Whether the phytochemicals are responsible for the risk reduction is unclear because people who consume such diets also tend to eat less fat, more fiber, and more foods containing vitamins C, D, and E. People who eat foods rich in a group of phytochemicals called flavonoids (found in red and purple grapes, red wine, and black teas) appear to have a lower risk of coronary artery disease. However, there is no clear cause-and-effect relationship. Some other factor in their life may account for the apparent lower risk.
A high-fiber diet is also recommended. There are 2 kinds of fiber:
Soluble fiber (which dissolves in liquid) is found in oat bran, oatmeal, beans, peas, rice bran, barley, citrus fruits, strawberries, and apple pulp. It helps lower cholesterol levels. It may decrease or stabilize high blood sugar (glucose) levels and increase low insulin levels. Thus, soluble fiber may help people with diabetes reduce their risk of coronary artery disease.
Insoluble fiber (which does not dissolve in liquid) is found in most grains and grain products and in fruits and vegetables such as apple skin, cabbage, beets, carrots, Brussels sprouts, turnips, and cauliflower. It also helps with digestive function.
Eating too much fiber, however, can interfere with the absorption of certain vitamins and minerals.
The diet should contain the recommended daily requirements of vitamins and minerals. Vitamin supplements are not considered an acceptable substitute for a healthy diet. The role of supplements in reducing the risk of coronary artery disease is somewhat controversial. Taking supplements of vitamin E or vitamin C does not seem to prevent coronary artery disease. Taking folate or vitamins B6 and B12 may lower homocysteine levels, but studies have not shown that taking these supplements decreases the risk of coronary artery disease.
Limiting the amount of simple sugar carbohydrates (such as refined white flour, white rice, processed foods) and increasing the proportion of whole grains may help reduce the risk of coronary artery disease because it reduces the risk of obesity and possibly of diabetes, which are also risk factors for coronary artery disease.
Overall, people should maintain a healthy weight and eat a variety of foods. Several specific diets have been proposed to reduce the risk of heart disease or stroke. The Mediterranean diet appears to reduce the risk of coronary artery disease as well as the risk of further heart attacks in those who already have heart disease. According to the American Heart Association, the Mediterranean diet consists of plenty of fruits, vegetables, nuts, seeds, bread and other grains, potatoes, beans, and olive oil. Dairy products, eggs, fish and poultry are eaten in low to moderate amounts. Fish and poultry are more common than red meat in this diet. It also centers on minimally processed, plant-based foods with fruit as a common dessert instead of sweets. Wine may be consumed in low to moderate amounts, usually with meals.
Types of Fat
There are 3 types of fat:
“Saturated” refers to the number of hydrogen atoms in a molecule of fat. Saturated fats contain as many hydrogen atoms as they can. They are usually solid at room temperature. Saturated fats are present in meats, dairy products, and artificially hydrogenated vegetable oils. The more solid the product, the higher is the proportion of saturated fats. A diet high in saturated fats promotes coronary artery disease. Unsaturated fats (monounsaturated and polyunsaturated) do not contain as many hydrogen atoms as they could. Monounsaturated fats could contain one more hydrogen atom. They are usually liquid at room temperature but start to solidify in the refrigerator. Olive oil and canola oil are examples. Polyunsaturated fats could contain more than one additional hydrogen atom. These fats are usually liquid at room and refrigerator temperatures. They tend to become rancid at room temperature. Corn oil is an example. Other polyunsaturated fats include omega-3 fats, contained in deep-sea fatty fish (such as mackerel, salmon, and tuna), and omega-6 fats, contained in vegetable oils. Trans fats are produced in a process called hydrogenation, in which hydrogen atoms are artificially added to polyunsaturated fats (“Trans” refers to where the hydrogen atoms are added to the fat molecule). Oils containing trans fats may be used to make food products that do not become rancid and to make solid fat products, such as margarine. Trans fats were previously used in commercial baked and fried foods, such as cookies, crackers, doughnuts, french fries, and other similar foods. Trans fats have been banned from use as an ingredient in the United States and many other nations. Trans fats increase low-density lipoprotein (LDL—the bad) cholesterol levels and decrease high-density lipoprotein (HDL—the good) cholesterol levels, and these effects appear to increase the risk of coronary artery disease. Thus, avoiding products that contain trans fats is wise. Trans fats are now listed on food labels. Also, if hydrogenated fat or partially hydrogenated fat is the first fat on the list of ingredients, the product contains trans fats. Some restaurants also provide information on which menu items contain trans fats. The appearance of a margarine or oil can also help identify foods containing these fats—the softer or more liquid, the lower the trans fat content. For example, the trans fat content of tub margarines is lower than that of stick margarines. Some margarine products contain a plant sterol or stanol, which can lower total and LDL cholesterol levels. Plant sterols and stanols may have this effect because they are not absorbed well in the digestive tract and they interfere with the absorption of cholesterol. These margarine products have been approved as heart healthy foods when they are used as part of a healthy diet. These products are made from unsaturated fat, contain less saturated fat than butter, and do not contain trans fats. However, they are expensive. The ideal combination of types of fats is unknown. However, a diet high in monounsaturated or omega-3 fats and low in trans fats is probably desirable. |
Physical inactivity
People who are physically active are less likely to develop coronary artery disease and high blood pressure. Exercise that promotes endurance (aerobic exercise such as brisk walking, bicycling, and jogging) or muscle strength (resistance training with free weights or weight machines) helps prevent coronary artery disease. Walking just 30 minutes each day can be beneficial. People who are out of shape or who have not exercised in a long time should consult their doctor before they start an exercise program.
Obesity
Modifying the diet and engaging in physical activity can help control obesity. Decreasing alcohol consumption can also help because alcohol is high in calories. A loss of even 10 to 20 pounds (4½ to 9 kilograms) can reduce the risk of coronary artery disease.
High cholesterol levels
High total and LDL (the bad) cholesterol levels can be lowered by exercising and by quitting smoking as well as by reducing the amount of fat in the diet. Medications that lower levels of total and LDL cholesterol in the blood (lipid-lowering drugs) may be used. The benefits of lowering cholesterol levels are greatest in people with other risk factors, such as smoking, high blood pressure, obesity, and physical inactivity.
Increasing the level of HDL (the good) cholesterol to healthy levels also helps reduce the risk of coronary artery disease. The same lifestyle changes that lower total and LDL cholesterol levels can help increase HDL cholesterol levels. Certain medications can also increase HDL levels, but it is not clear whether using medications to increase HDL levels is helpful. For people who are overweight, losing weight can also help.
High blood pressure
Lowering high blood pressure reduces the risk of coronary artery disease. Treatment of high blood pressure begins with lifestyle changes: eating a healthy diet that is low in salt and, if needed, losing weight and increasing physical activity. Medication therapy may also be necessary.
Diabetes mellitus
Good control of diabetes mellitus reduces the risk of some complications of diabetes, but the effects of such control on the development of coronary artery disease are less clear. Good control of diabetes may also reduce the risk of complications of coronary artery disease.
Aspirin
Aspirin, which had been recommended in the past for people who have never had coronary artery disease, is not currently recommended for most such people.







