


An aortic dissection is an often fatal disorder in which the inner layer (lining) of the aortic wall tears and separates from the middle layer of the aortic wall.
Most aortic dissections occur because high blood pressure causes the artery’s wall to deteriorate.
People have sudden, excruciating pain, most commonly across the chest but also in the back between the shoulder blades.
Doctors do imaging studies to confirm the diagnosis.
People usually take medications to decrease blood pressure, and doctors do surgery to repair the tear or place stent grafts to cover the tear.
(See also Overview of Aortic Aneurysms and Aortic Dissection.)
The aorta is the largest artery of the body. It receives oxygen-rich blood from the heart and distributes it to the body through smaller arteries that branch off of it. The thoracic aorta, where most aortic dissection occurs, is the part of the aorta that passes through the chest.
When the lining of the aorta tears, blood can push through the tear, separating (dissecting) the middle layer of the wall from the still intact outer layer. As a result, a new, false channel forms in the wall of the aorta. As the aortic dissection lengthens along the aorta, it can close off the points at which one or more arteries branch off from the aorta, blocking blood flow.
Aortic dissections are three times more common among men and are more common among people of African ancestry (specifically African-American people) and less common among people with Asian ancestry. About three fourths of aortic dissections occur in people aged 40 to 70 years.
The most common cause of aortic dissection is
Deterioration of the artery's wall because of longstanding high blood pressure
More than two thirds of people who have an aortic dissection have high blood pressure.
Less common causes of aortic dissection include
Hereditary connective tissue disorders, especially Marfan syndrome and Ehlers-Danlos syndrome
Birth defects of the heart and blood vessels, such as coarctation (narrowing) of the aorta, patent ductus arteriosus (a connection between the aorta and the pulmonary artery), and defects of the aortic valve
Injury such as a car crash or fall causing a strong blow to the chest
Aging, which can cause deterioration of the artery's wall
Rarely, a dissection occurs accidentally when doctors are inserting a catheter into an artery (for example, during aortography or angiography) or doing surgery on the heart or blood vessels.
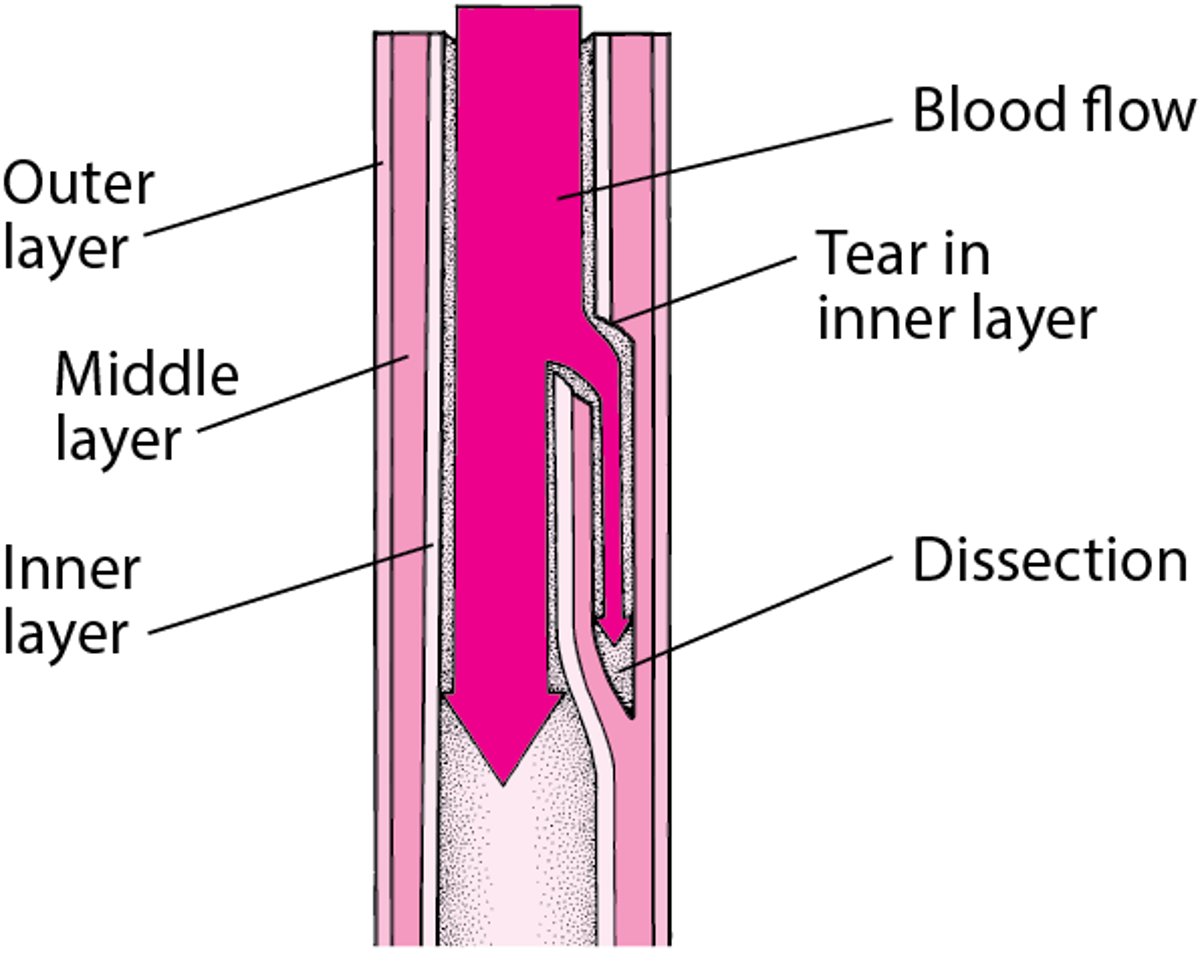
Understanding Aortic Dissection
In an aortic dissection, the inner layer (lining) of the aortic wall tears, and blood surges through the tear, separating (dissecting) the middle layer from the outer layer of the wall. As a result, a new, false channel forms in the wall. |

Symptoms of Aortic Dissection
More than 90% of people who have an aortic dissection experience pain—typically sudden, excruciating pain, often described as tearing or ripping. Some people may faint as a result of the pain. Most commonly, the pain is felt across the chest but is often also felt in the back between the shoulder blades. The pain frequently travels along the path of the dissection as it advances along the aorta. Thus, people may have abdominal pain or lower back pain if the mesenteric arteries, which supply the intestines, are blocked.
Complications of aortic dissection
Complications include
Stroke (if the cerebral arteries, which supply the brain, are blocked)
Heart attack (if the coronary arteries, which supply the heart muscle, are blocked)
Kidney failure (if the renal arteries, which supply the kidneys, are blocked)
Nerve and/or spinal cord damage that causes tingling or an inability to move a limb (if the spinal arteries are blocked)
Blood may leak from the dissection and accumulate in the chest. Blood leaking from a dissection near the heart may enter the pericardial space (between the two layers of membranes that surround the heart), preventing the heart from filling properly and causing cardiac tamponade—a life-threatening disorder.
A dissection that involves the first few inches of the aorta (ascending aorta) closest to the heart may affect the attachments of the aortic valve, the heart valve that keeps blood from flowing back into the heart. If the aortic valve attachments are weakened, the valve can leak, causing heart failure.
Diagnosis of Aortic Dissection
Imaging tests such as CT angiography, magnetic resonance angiography, or transesophageal echocardiography
The distinctive symptoms of an aortic dissection often make the diagnosis obvious to doctors, although the disorder causes a variety of symptoms that sometimes resemble those of other disorders. In some people with aortic dissection, pulses in the arms and legs are diminished or absent. Depending on the location of the dissection along the aorta, there may be a difference in blood pressure between the right and left arm. A dissection that is moving toward the heart may cause a murmur that can be heard through a stethoscope.
Chest x-rays are the first step in detecting aortic dissection. X-rays show a widened aorta in 90% of people with symptoms. However, this finding may be due to other disorders. Computed tomography (CT) angiography, done after injecting a contrast agent, can quickly and reliably detect aortic dissection and thus is useful in an emergency. Transesophageal echocardiography or magnetic resonance angiography can also reliably detect aortic dissections, even very small ones.
Treatment of Aortic Dissection
Medications to control blood pressure
Surgery or sometimes an endovascular stent graft
People with an aortic dissection are admitted to an intensive care unit, where their vital signs (pulse, blood pressure, and rate of breathing) are closely monitored. Death can occur a few hours after an aortic dissection begins. Therefore, as soon as possible, medications are given intravenously to reduce the heart rate and blood pressure to the lowest level that can maintain a sufficient blood supply to the brain, heart, and kidneys. The lower heart rate and blood pressure help limit the spread of the dissection. Soon after medication therapy begins, doctors must decide whether to recommend surgery or to continue giving medications instead of doing surgery.
Doctors almost always recommend surgery for dissections that involve the first few inches of the aorta (ascending aorta) closest to the heart, unless complications of the dissection make the risk of surgery too high. During surgery, surgeons remove the largest possible area of dissected aorta, close the channel that was torn between the middle and outer layers of the aorta’s wall, and rebuild the aorta with a synthetic graft. If the aortic valve is leaking, surgeons repair or replace it.
For dissections in the aorta farther from the heart (descending aorta), doctors usually continue medication therapy without surgery or consider placement of an endovascular stent graft, To do an endovascular stent graft procedure, doctors thread a long, thin wire through the large artery in the groin (femoral artery) and up to the dissecting area. Then they slide the stent graft, which is a hollow tube like a collapsible straw, over the wire and inside the damaged area of the aorta. Then the stent graft is opened, forming a stable channel for blood flow. This procedure takes 2 to 4 hours, and the hospital stay is usually 1 to 3 days. Stent grafts, which are less invasive than open surgery, have improved the survival rate and lowered the risk of complications for people with dissections of the descending aorta.
Surgery or a stent graft repair is always necessary if the dissection causes the artery to leak blood, blocks the blood supply to the legs or to vital organs in the abdomen, causes symptoms, is enlarging, or occurs in a person with Marfan syndrome.
All people who have an aortic dissection, including those treated surgically, have to take medications to keep their blood pressure down, usually for the rest of their lives. Such therapy helps reduce stress on the aorta. Medication therapy to lower blood pressure usually consists of a beta-blocker or calcium channel blocker plus another antihypertensive drug such as an angiotensin-converting enzyme (ACE) inhibitor. Cholesterol-lowering drugs and diet modification are used if the person has atherosclerosis.
Doctors watch closely for complications that can occur in people who have had an aortic dissection. The most important are
Another dissection
Development of aneurysms in the weakened aorta
Increasing leakage backward through the aortic valve
Any of these complications may require surgical repair.
Prognosis for Aortic Dissection
About 20% of people who have an aortic dissection die before they reach the hospital.
Without treatment, the death rate is high within the first 2 weeks and varies depending on the location of the dissection. With treatment, about 70% of people who have dissection of the first part of the aorta and about 90% of those who have dissection of the aorta farther from the heart survive to leave the hospital. About 60% of people who survive the first 2 weeks are still alive 5 years after treatment, and 40% live at least 10 years. Of people who survive more than 2 weeks, one third eventually die of complications of the dissection, and the other two thirds die of other disorders.







