


A breast mass (lump) may be discovered by patients incidentally or during breast self-examination or by the clinician during physical examination.
Masses may be painless or painful and are sometimes accompanied by a nipple discharge or skin changes.
Etiology of Breast Masses
All breast masses must be evaluated to exclude breast cancer, but the majority are nonmalignant. The most common causes include
Fibrocystic changes
Fibroadenomas
Fibrocystic changes (previously, fibrocystic breast disease) refers to nonproliferative lesions, including breast cysts and nondescript masses (usually in the upper outer part of the breast); these findings may occur in isolation or together. Breasts have a nodular and dense texture and are frequently tender when palpated. The breasts may feel heavy and uncomfortable. Women may feel a burning pain in the breasts. Fibrocystic changes are the cause of the most commonly reported breast symptoms. Symptoms tend to subside after menopause.
Repeated stimulation by estrogen and progesterone may contribute to the development of fibrocystic changes, which are more common among women who had early menarche, who had their first live birth at age > 30, or who are nulliparous. Fibrocystic changes are not associated with increased risk of cancer.
Fibroadenomas are typically smooth, rounded, mobile, painless masses; they may be mistaken for cancer. They usually develop in women during their reproductive years and may decrease in size over time. Simple fibroadenomas do not appear to have an increased risk of breast cancer. Complex fibroadenomas are associated with a slightly increased risk of breast cancer (1). Juvenile fibroadenomas are a variant that occur in adolescents, and unlike fibroadenomas in older women, these fibroadenomas continue to grow over time.


GIRAND/SCIENCE PHOTO LIBRARY
Breast infections (mastitis) cause pain, erythema, and swelling; an abscess can produce a discrete mass. Puerperal mastitis, usually due to Staphylococcus aureus, can cause massive inflammation and severe breast pain, sometimes with an abscess. Infections are extremely rare except during the puerperium (postpartum) or after penetrating trauma. They may occur after breast surgery. If infection occurs under other circumstances, an underlying cancer should be sought promptly. Types of benign nonlactational mastitis are periductal mastitis, idiopathic granulomatous mastitis, and tuberculous mastitis (see Extrapulmonary Tuberculosis); these types occur mainly in young women.


MID ESSEX HOSPITAL SERVICES NHS TRUST/SCIENCE PHOTO LIBRARY
Galactocele is a round, easily movable milk-filled cyst that usually occurs up to 6 to 10 months after lactation stops. Such cysts rarely become infected.


DR M.A. ANSARY/SCIENCE PHOTO LIBRARY
Cancers of various types can manifest as a mass.
Etiology reference
1. Nassar A, Visscher DW, Degnim AC, et al: Complex fibroadenoma and breast cancer risk: a Mayo Clinic Benign Breast Disease Cohort Study. Breast Cancer Res Treat 153(2):397-405, 2015. doi:10.1007/s10549-015-3535-8
Evaluation of Breast Masses
History
History of present illness should include how long the mass has been present, whether the size is constant or varies, and whether the mass is painful. Previous occurrence of a mass and the outcome of its evaluation should be queried.
Review of systems should determine whether nipple discharge is present and, if present, whether it is unilateral, spontaneous or only in response to breast manipulation and whether it is clear, milky, or bloody. Symptoms of advanced cancer (eg, weight loss, malaise, bone pain) should be sought.
Past medical history should include risk factors for breast cancer, including previous diagnosis of breast cancer, history of radiation therapy to the chest area before age 30 (eg, for Hodgkin lymphoma). Family history should note breast cancer in a 1st-degree relative (mother, sister, daughter) and, if family history is positive, whether the relative carried one of the inherited gene mutations that predispose to breast cancer (eg, BRCA1, BRCA2).
Physical examination
Examination focuses on the breast and adjacent tissue. The breast is inspected for skin changes over the area of the mass, nipple inversion (retraction), and nipple discharge. Skin changes may include erythema, eczematous appearance, edema, or dimpling (sometimes termed peau d’orange [orange peel]).


SCIENCE PHOTO LIBRARY
The mass is palpated for size, tenderness, consistency (ie, hard or soft, smooth or irregular), borders (well-defined or nondiscrete), and mobility (whether it feels freely mobile or fixed to the skin or chest wall).
The axillary, supraclavicular, and infraclavicular areas are palpated for masses and adenopathy.
Red flags
Certain findings are of particular concern:
Mass fixed to the skin or chest wall
Stony hard, irregular mass
Skin dimpling
Thickened, erythematous skin
Bloody or spontaneous nipple discharge
Matted or fixed axillary lymph nodes
Interpretation of findings
Painful, tender, rubbery masses in women who have a history of similar findings and who are of reproductive age suggest fibrocystic changes.
Red flag findings suggest cancer. However, the characteristics of benign and malignant lesions, including presence or absence of risk factors, overlap considerably. For this reason and because failure to recognize cancer has serious consequences, patients require testing to exclude breast cancer more conclusively.
Testing
Initially, physicians try to differentiate solid from cystic masses because cysts are rarely cancerous. Typically, ultrasonography is done first. Lesions that appear cystic may be aspirated (eg, when they cause symptoms).
Fluid aspirated from a cyst is sent for cytology if
It is turbid or grossly bloody.
Minimal fluid is obtained.
A mass remains after aspiration.
If these findings are present, mammography followed by imaging-guided core needle biopsy is done.
Patients are reexamined in 4 to 8 weeks. If the cyst is no longer palpable, it is considered benign. If the cyst has recurred, it is reaspirated, and any fluid is sent for cytology regardless of appearance. A third recurrence or persistence of the mass after initial aspiration (even if cytology was negative) requires biopsy.
Solid masses are evaluated with mammography followed by imaging-guided core needle biopsy. Surgical biopsy is done if image-guided biopsy is not possible because the lesion is too close to the skin or chest wall, if the patient cannot maintain the position needed for needle biopsy, or if the patient prefers surgical biopsy.

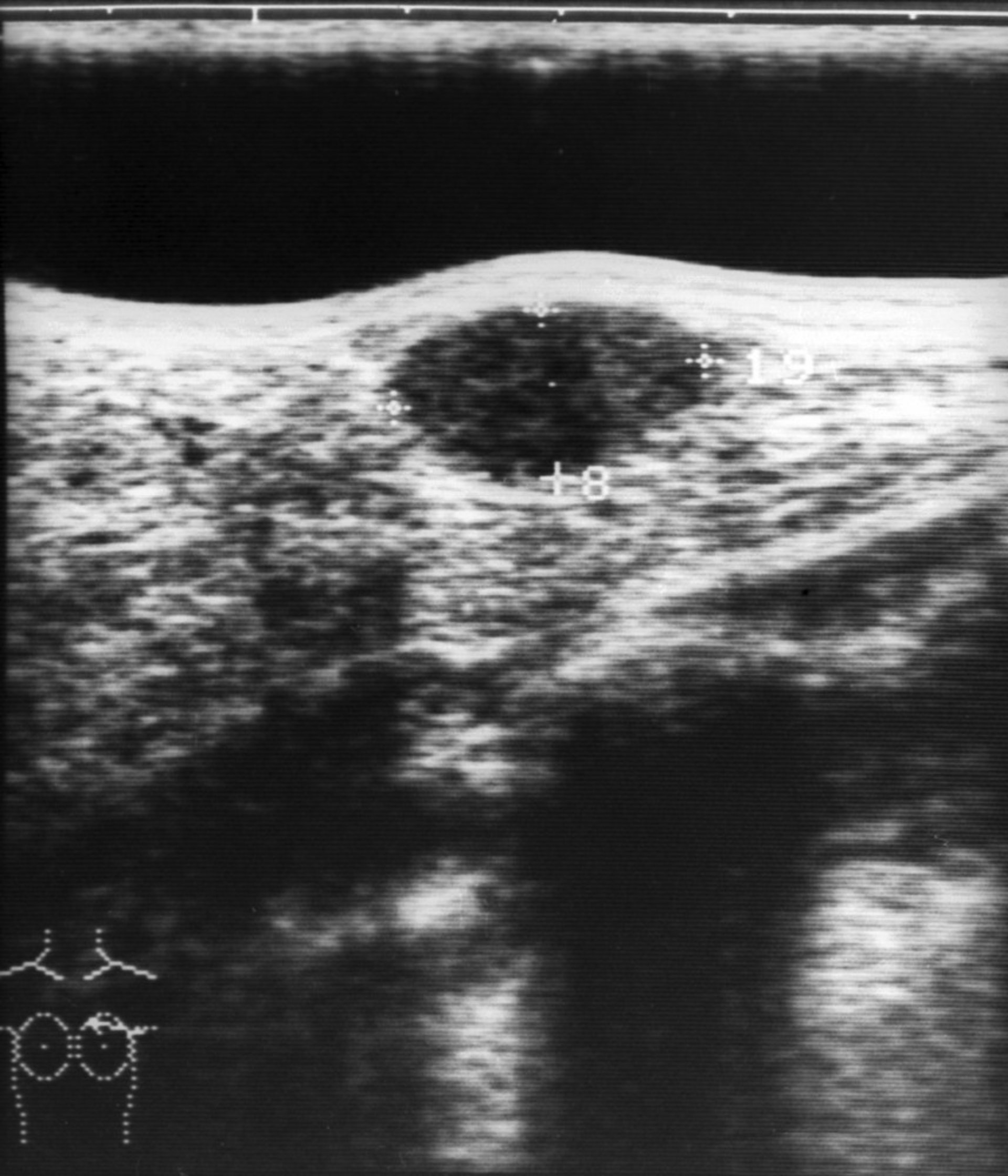
ZEPHYR/SCIENCE PHOTO LIBRARY

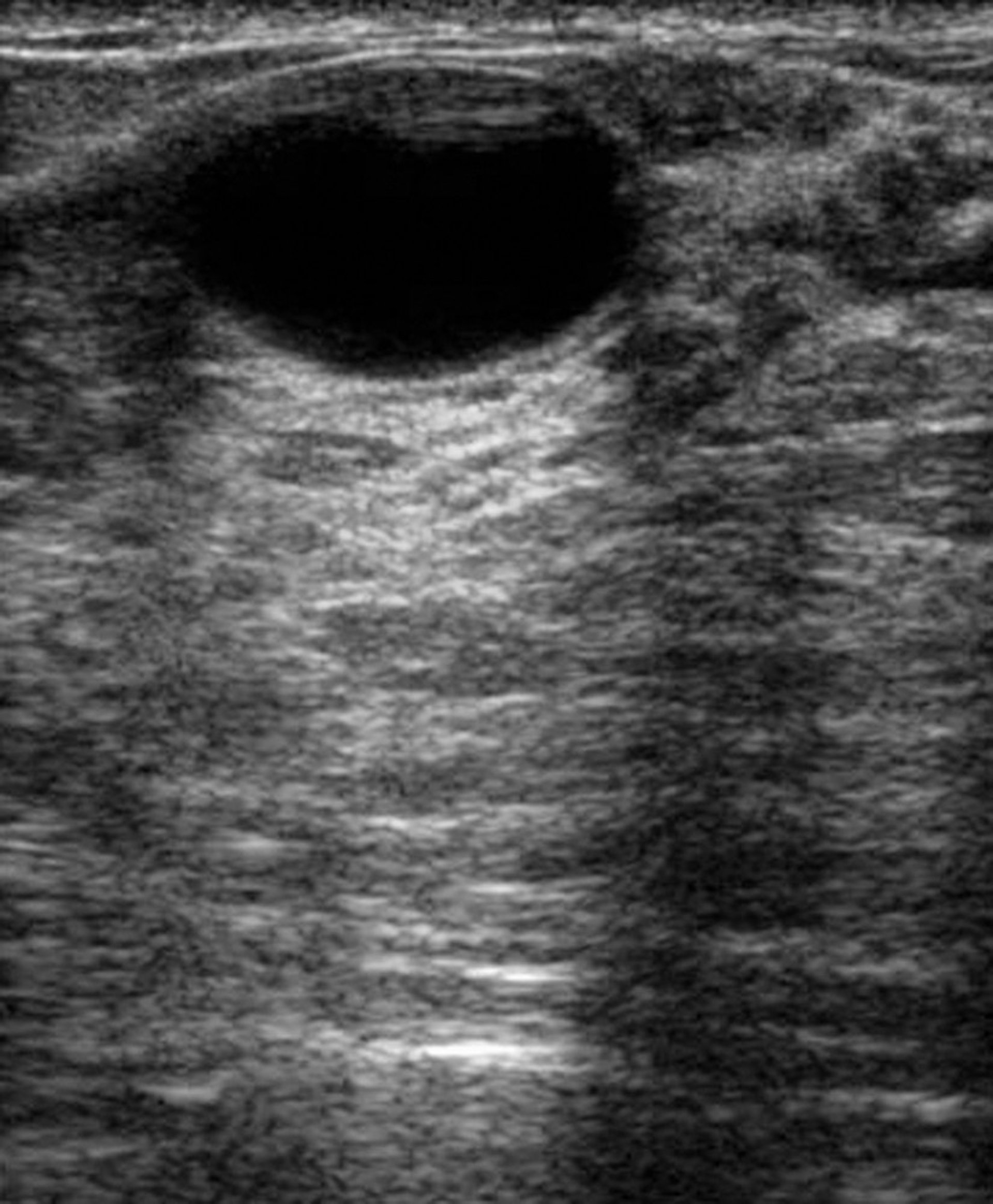
DR NAJEEB LAYYOUS/SCIENCE PHOTO LIBRARY
Treatment of Breast Masses
Treatment of a breast mass is directed at the cause.
A fibroadenoma is usually removed if it grows or causes symptoms. Fibroadenomas can usually be surgically excised or, if < 3 cm, cryoablated after patients are given a local anesthetic, but fibroadenomas frequently recur. The American Society of Breast Surgeons recommends that adenomas be excised if they have any of the following features: stromal mitoses, stromal overgrowth, nuclear pleomorphism, fragmentation, or adipose tissue infiltration (1). Patients who have fibroadenomas that are not excised should be checked periodically for changes. After patients have had several fibroadenomas established as benign, they may decide against having subsequent ones excised. Because juvenile fibroadenomas tend to grow, they should be removed solely because they increase in size.
Acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs), and athletic bras (to reduce trauma) can be used to relieve symptoms of Acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs), and athletic bras (to reduce trauma) can be used to relieve symptoms offibrocystic changes. Evening primrose oil may be somewhat effective.
A galactocele typically resolves after aspiration.
Breast cancer is treated as appropriate.
Treatment reference
1. The American Society of Breast Surgeons: Consensus guideline on concordance assessment of image-guided breast biopsies and management of borderline or high-risk lesions; 2016. Accessed December 18, 2023.
Key Points
Most breast masses are not cancer.
Breast masses are usually evaluated first with ultrasonography.
Cystic masses are aspirated and require further evaluation if the fluid is turbid or bloody, minimal fluid is obtained, or the mass does not resolve.
Solid masses are evaluated with mammography and biopsy.







